Medical Emergency Equipment for Dental Practices: The Ultimate 2026 Compliance Checklist

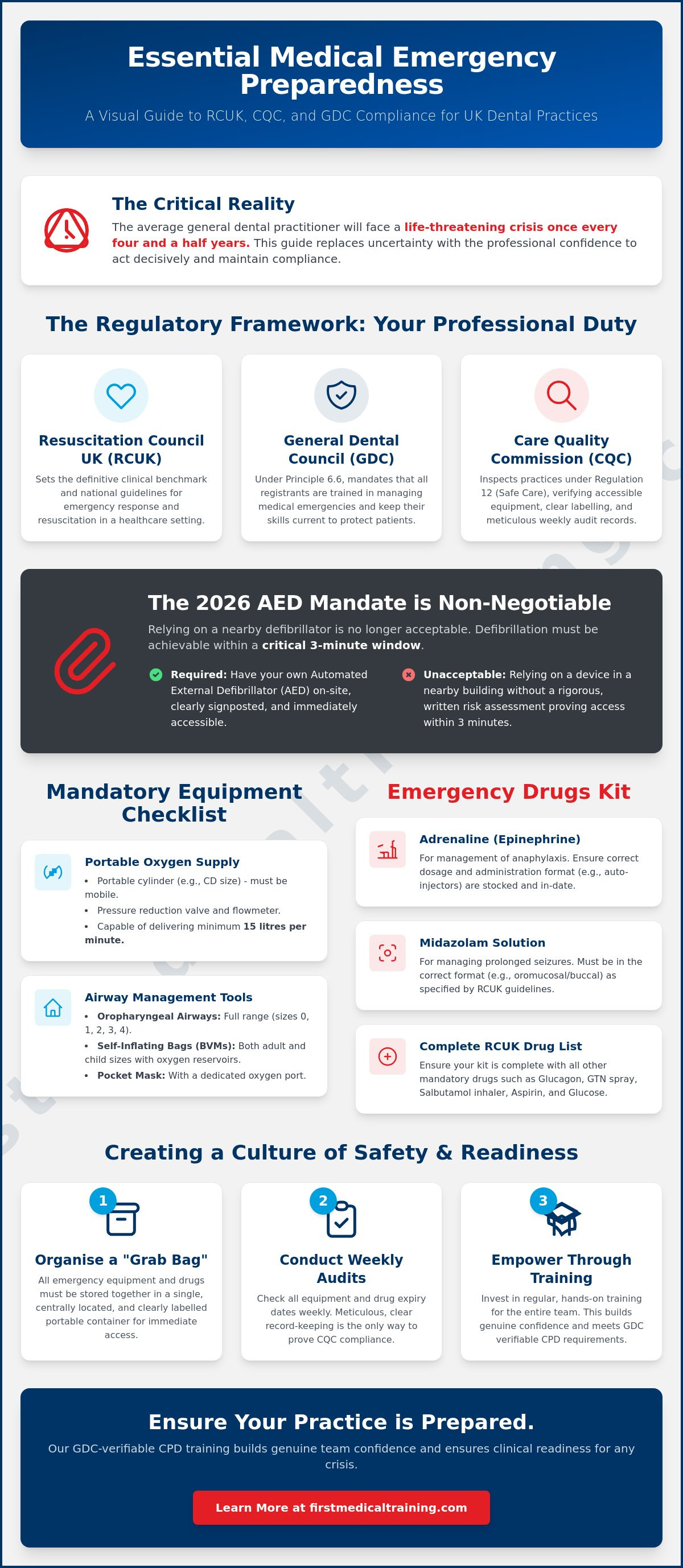
Did you know that the average general dental practitioner will face a life-threatening crisis once every four and a half years? While these events are infrequent, the responsibility to maintain the correct medical emergency equipment dental practice standards is a constant pressure. You've likely felt that familiar anxiety when auditing expiry dates on adrenaline injectors or questioned whether your AED pads are still compliant with the latest 2026 CQC expectations. It's natural to feel concerned about the technicality of Resuscitation Council (UK) guidelines, particularly when your professional reputation and patient safety are on the line.
We've created this guide to replace that uncertainty with absolute, professional confidence. You'll gain access to a definitive checklist covering every mandatory drug and piece of equipment required for GDC compliance. We'll outline the specific requirements for everything from oropharyngeal airways to midazolam solution, ensuring your kit is audit-ready and your team feels empowered to act. This is your roadmap to a well-led surgery where every member of staff knows their role and has the tools to save a life.
Key Takeaways
- Understand how to align your surgery with the latest Resuscitation Council (UK) standards and CQC inspection requirements for 2026.
- Identify the mandatory medical emergency equipment dental practice settings must have on-site, including portable oxygen and specific airway management tools.
- Master the essential pharmaceutical list, including correct dosages and administration formats for adrenaline and midazolam, to ensure your kit is audit-ready.
- Learn the "Grab Bag" philosophy and the protocol for weekly equipment checks to prevent the common pitfall of expired or missing life-saving tools.
- Discover how to meet GDC verifiable CPD requirements through training that builds genuine team confidence and clinical readiness for a crisis.
The Regulatory Framework: GDC and CQC Requirements for 2026
The regulatory landscape for UK dentistry is clear. The Resuscitation Council UK (RCUK) sets the clinical benchmark for emergency response. Both the Care Quality Commission (CQC) and the General Dental Council (GDC) treat these standards as the definitive requirement for any surgery. Staying compliant isn't just about ticking a box; it's about ensuring your team can act decisively when a patient's life is at risk. When we consider what constitutes a dental emergency, it often involves pain or trauma, yet systemic medical crises like anaphylaxis or cardiac arrest can occur in any clinical setting. This is why having the correct medical emergency equipment dental practice kit on hand is non-negotiable.
The GDC expects every dental professional to be competent in managing medical emergencies. This requirement is reinforced by the CQC, which inspects practices under the "Safe" and "Well-led" domains. A central part of this inspection involves verifying that you have immediate access to an Automated External Defibrillator (AED). In 2026, relying on a defibrillator located in a nearby shop or pharmacy is no longer acceptable. If your practice doesn't have its own AED, you must provide a rigorous, written risk assessment explaining how you'll achieve defibrillation within the critical three-minute window. Without this, you're failing to meet the basic safety standards expected of a modern clinical environment.
GDC Standards and Professional Indemnity
GDC Principle 6.6 requires all registrants to be trained in medical emergencies and to keep their skills up to date. This isn't a suggestion; it's a professional obligation. If you can't demonstrate that you've maintained your skills and medical emergency equipment dental practice standards, your professional registration could be at risk. Most indemnity providers also base their coverage on the assumption that you're following RCUK guidelines. Failing an audit or, worse, failing to respond correctly in a crisis, could leave you legally and professionally exposed. Every member of the team, from the lead clinician to the newest trainee nurse, must know exactly where the emergency kit is and how to use every item within it.
CQC Regulation 12: Safe Care and Treatment
CQC inspectors focus heavily on Regulation 12. They'll look for evidence that your equipment is centrally located, clearly labelled, and easily accessible. A common mistake is keeping the AED or oxygen in a locked office or a cluttered storage area. If you share an AED with another building, your documentation must prove that it's reachable and ready for use in seconds. Inspectors will also check your training logs and your weekly equipment audit records. They want to see a culture of safety where checks are performed religiously. Meticulous record-keeping is the only way to prove to an inspector that your equipment is consistently functional and that your drugs are within their expiry dates.
Essential Medical Emergency Equipment Checklist
Every clinical room in your surgery must have immediate access to a standardised set of hardware designed to support life until an ambulance arrives. The core of this kit is your medical oxygen supply. You need a portable cylinder, typically a CD size, equipped with a pressure reduction valve and a flowmeter capable of delivering at least 15 litres per minute. It's a common oversight to rely on chairside oxygen, but your emergency supply must be mobile. Following the Emergency drugs and equipment guidelines ensures that your hardware meets the rigorous standards expected during a clinical crisis.
Airway management is the next priority. Your kit must include a full range of oropharyngeal airways, specifically sizes 0, 1, 2, 3, and 4. These allow you to maintain a patent airway in patients of all ages. For ventilation, you're required to have self-inflating bags (often called Bag Valve Masks or BVMs) with oxygen reservoirs. You must stock both adult and child sizes to remain compliant. A pocket mask with an oxygen port is also essential for those initial moments before the BVM is deployed. Having the right medical emergency equipment dental practice kit means these tools are organised and ready to use in seconds, not buried under boxes of PPE.
Your Automated External Defibrillator (AED) is perhaps the most critical piece of technology in the building. Modern units should provide clear voice prompts to guide the user through the process. It's now a standard expectation that your AED is registered with "The Circuit", the national defibrillator network. This ensures that emergency services know exactly where your device is located. Regular battery and pad checks are vital; pads usually have a two year shelf life and must be replaced before they expire to ensure the conductive gel remains effective.
Oxygen Delivery and Suction Requirements
High-concentration reservoir masks are necessary for patients who are breathing but require supplemental oxygen. These are different from standard nasal cannulas and are vital for managing conditions like anaphylaxis or myocardial infarction. Equally important is your portable suction. While your dental chair has suction, a portable, independently powered unit is mandatory. It must include a Yankauer catheter and be capable of clearing the airway if a patient vomits or has a significant bleed. If the power fails, your chairside suction won't work, but your portable unit will save lives.
Supplemental Life-Saving Technology: LifeVac
Standard choking protocols involve back blows and abdominal thrusts, but these aren't always effective or possible, especially with patients in a dental chair or those with physical disabilities. This is why many UK practices are now choosing to include the LifeVac Anti-Choking Device in their waiting rooms and surgeries. It's a non-invasive suction device that can clear an airway obstruction when traditional methods fail. Integrating this technology into your practice provides an extra layer of safety for both patients and visitors. It's a simple addition that offers immense peace of mind to a team that wants to be prepared for every eventuality.
The Emergency Drugs Kit: Mandatory Medications
While the previous section focused on essential hardware, the pharmaceutical element of your medical emergency equipment dental practice kit is what facilitates life-saving intervention. The Resuscitation Council UK (RCUK) specifies a core list of drugs that every clinical setting must hold. This includes Adrenaline (1:1000, 1mg/mL), dispersible Aspirin (300mg), Glucagon (1mg), Glucose for oral administration, Glyceryl Trinitrate (GTN) spray, and Midazolam oromucosal solution. It's also mandatory to stock a Salbutamol inhaler accompanied by a spacer device. Spacers are critical because patients in respiratory distress often struggle to coordinate their breathing with a standard puffer.
Effective clinical protocols for Managing dental emergencies depend on the immediate availability of these drugs. One often overlooked area is the "cold chain" for Glucagon. While Glucagon can be stored at room temperature, its shelf life is significantly reduced compared to refrigerated storage. You must check the manufacturer's instructions; usually, room temperature storage limits the lifespan to 18 or 24 months. If you store it in the fridge, ensure it's easily accessible and that the team knows exactly where to find it during a crisis.
Emergency Drug Protocols for Common Scenarios
In cases of anaphylaxis, the early administration of intramuscular adrenaline is the single most important step. Your kit should contain at least two ampoules or auto-injectors to allow for a second dose if the patient doesn't improve. For hypoglycaemia, oral glucose is the first choice if the patient is conscious and able to swallow. However, if they become unconscious, injectable glucagon must be used. For cardiac chest pain, the protocol involves one or two sprays of GTN under the tongue followed by a single 300mg dispersible aspirin, which the patient should chew to speed up absorption.
Managing Drug Expiry and Stock Rotation
A robust monthly audit system is the only way to avoid the risk of discovering an expired drug during a real emergency. Don't just look at the month; record the exact date and batch number for every item. This practice allows you to track potential manufacturer recalls more efficiently. When a drug expires, it must be disposed of via a licensed pharmaceutical waste contractor. Keeping expired drugs in your "Grab Bag" is a major red flag for CQC inspectors and compromises patient safety. Rotate your stock so that the items with the shortest lifespan are always at the front of your kit.
Maintenance, Audits, and Common Mistakes in Surgery
Success in a medical emergency depends as much on organisation as it does on clinical skill. Many surgeries make the mistake of storing their medical emergency equipment dental practice kit in various cupboards or drawers across the building. This fragmented approach causes delays and confusion during a crisis. Instead, we advocate for the "Grab Bag" philosophy. Every mandatory item, from your oxygen cylinder to your adrenaline ampoules, should be stored in one portable, high-visibility bag. This allows a single team member to bring the entire life-saving kit to the patient in seconds.
To address the "human factor" of high-stress response, consider organising the internal compartments of your grab bag with colour-coded pouches. For example, using a red pouch for cardiac emergencies and a blue one for respiratory distress helps the team find the correct tools without having to dig through unrelated items. This simple system reduces cognitive load, allowing the clinician to focus entirely on the patient. If you want to ensure your staff are fully competent in these organisational protocols, our Medical Emergencies in a Dental Practice Course provides the practical foundation your team needs.
Common CQC failures often stem from small but significant oversights. Inspectors frequently find uncharged portable suction units or missing child-sized reservoir masks. Whilst your primary patient base might be adults, the regulatory requirement to be prepared for all ages is absolute. Your audit schedule must be split into weekly and monthly tasks. Oxygen levels and AED battery status require a weekly check, whilst drug expiry dates and batch numbers can be audited monthly. These checks aren't just a regulatory hurdle; they're your primary defence against equipment failure when a life is on the line.
Creating an Audit Trail for Clinical Governance
A robust audit trail is the backbone of "well-led" clinical governance. You should maintain a simple, dedicated logbook where every check is signed and dated. If a piece of equipment fails or a drug reaches its expiry, the log must document the corrective action taken, such as the date a replacement was ordered. Appointing a "Lead for Medical Emergencies" ensures that one person carries the responsibility for these checks, preventing the "bystander effect" where everyone assumes someone else has checked the oxygen.
AED Maintenance and Pad Replacement
Your AED requires a 10-second daily visual check to ensure the status indicator is green. This simple habit prevents the nightmare scenario of a flat battery during a cardiac arrest. Always keep a spare set of adult pads and a "prep kit" containing a razor, scissors, and gloves attached to the AED. For practices that treat children, ensure you have paediatric pads or a device with a paediatric switch. Remember that pad adhesive degrades over time; even if unused, they must be replaced every two years to ensure they will stick to the patient's chest correctly.
Beyond the Kit: Training and Team Readiness
The most sophisticated medical emergency equipment dental practice settings can buy is ultimately a collection of plastic and pharmaceuticals until it's placed in the hands of a competent responder. Clinical readiness is a marriage of hardware and high-quality education. Without regular, hands-on practice, the stress of a real-life crisis can lead to hesitation or incorrect use of life-saving tools. This is why Dental Immediate Life Support (ILS) Training is so vital. It bridges the gap between having the kit and knowing exactly how to deploy it under pressure.
The GDC recommends that dental professionals complete at least 10 hours of verifiable CPD in medical emergencies every five-year cycle. We suggest a minimum of two hours per year to keep these skills sharp. Whilst external courses are valuable, there's immense benefit in conducting training within your own surgery. Practising with your own oxygen cylinders and your specific AED model ensures that every staff member knows the exact location and operation of your kit. Running "mock emergencies" or "crash drills" allows your team to test communication and identify any bottlenecks in your response plan before a real incident occurs. For broader workplace protection, working with a specialist like Guardian Safety can help you integrate these clinical protocols into a wider health and safety strategy.
The Human Element: Mental Health First Aid
A medical emergency doesn't end when the ambulance leaves. The psychological impact on the dental team can be significant, often leading to post-incident anxiety or a loss of clinical confidence. Effective debriefing protocols are essential for learning from the event without assigning blame. Increasingly, forward-thinking surgeries are recognising that Mental Health First Aid for Dental Practices is a crucial component of staff wellbeing. Supporting your team's mental resilience ensures they remain capable and ready to serve their patients, even after the most challenging clinical days.
Choosing the Right Training Partner
When selecting an education provider, look for an accredited partner with deep roots in the dental sector. Your trainer should understand the specific constraints of a dental surgery and provide GDC-compliant certification. A comprehensive Medical Emergencies in a Dental Practice Course should involve the whole team, from receptionists to lead clinicians. This collective approach ensures that if a patient collapses in the waiting room, the first person on the scene is just as prepared as the dentist in the chair. Is your practice truly ready for an emergency today? If you have the kit, the drugs, and a trained team, the answer is a confident yes.
Building a Culture of Clinical Readiness
Maintaining the correct medical emergency equipment dental practice standards is a continuous commitment to patient safety and professional excellence. By implementing a robust "Grab Bag" system, conducting weekly audits, and ensuring your pharmaceutical kit adheres to 2026 RCUK guidelines, you remove the anxiety of CQC inspections. Hardware and drugs provide the foundation, but a truly safe practice is defined by a team that can act without hesitation. The ultimate goal is to ensure that your equipment and your people work in perfect harmony during those critical first minutes of a crisis.
We've spent two decades since our founding in 2006 refining dental training to meet the exact needs of modern surgeries. As specialist suppliers of the LifeVac anti-choking device and providers of accredited Dental ILS and EFAW courses, we bridge the gap between regulatory requirements and real-world skills. Our mission is to transform your compliance checklist into genuine clinical confidence. We understand the unique pressures of the dental environment and provide the steady, reliable support you need to stay compliant.
Book your team onto an accredited Medical Emergencies in a Dental Practice Course today and ensure your surgery is prepared for any eventuality. With the right tools and the right training, you can focus on what you do best: providing exceptional dental care in a safe, professional environment.
Frequently Asked Questions
What medical emergency drugs are mandatory for a UK dental practice?
The mandatory list includes Adrenaline (1:1000), Aspirin (300mg), Glucagon, Glucose, GTN spray, Midazolam solution, Medical Oxygen, and Salbutamol. These must be kept in a standardised medical emergency equipment dental practice kit to ensure they're ready for immediate use. You should also ensure you have a spacer device for the salbutamol inhaler. These specific drugs represent the minimum requirement for managing crises like anaphylaxis, cardiac chest pain, or asthma attacks in a clinical setting.
Do I need a defibrillator if there is one in the building next door?
You must have an AED on-site unless a robust risk assessment proves that a device in a neighbouring building is accessible within a three-minute window. The GDC and CQC prioritise immediate access, as survival rates from cardiac arrest drop by 10% for every minute of delay. Relying on an external device is often considered high-risk. Most practices find that having their own unit is the only way to guarantee they meet the required response times.
How often should we check our emergency oxygen cylinders?
You should conduct and log checks on your emergency oxygen cylinders every week. This check must verify that the cylinder is full enough to deliver at least 15 litres per minute for the duration of an emergency. You should also check the integrity of the seals and the expiry date of the cylinder itself. Documenting these weekly checks in a dedicated logbook provides the audit trail that CQC inspectors expect to see during a practice visit.
Is the LifeVac anti-choking device mandatory for GDC compliance?
The LifeVac anti-choking device is not currently a mandatory requirement for GDC compliance, but it is highly recommended as supplemental equipment. It provides a non-invasive solution for clearing airway obstructions when standard back blows or abdominal thrusts are unsuccessful or impossible to perform. Many surgeries include it in their waiting rooms to protect patients with complex needs or those for whom traditional choking protocols might be physically difficult to execute.
What is the difference between BLS and ILS training for dental teams?
BLS focuses on high-quality CPR and the use of an AED, whilst ILS training includes more advanced skills such as airway adjuncts and drug administration. ILS is designed to empower the dental team to manage a patient until the ambulance arrives, often including roles for team leaders and more technical equipment. While BLS is the minimum standard, ILS is increasingly preferred for clinical teams to ensure a more comprehensive level of emergency preparedness.
Can a dental nurse administer emergency drugs in a crisis?
Dental nurses can legally administer certain emergency drugs, such as adrenaline, under the "administration in an emergency" exemptions of the Human Medicines Regulations 2012. In a crisis, the priority is the patient's survival. Nurses should act within their competence and under the direction of the prescribing clinician whenever possible. Regular team training ensures that every member of staff feels confident and legally protected when administering life-saving medications during a medical emergency.
How should we store Glucagon in the dental surgery?
Glucagon should ideally be stored in a refrigerator between 2°C and 8°C to maintain its full shelf life as stated by the manufacturer. If you choose to store it at room temperature (up to 25°C), the lifespan is typically reduced to 18 months, and you must mark the new expiry date clearly on the box. It's vital that the team knows exactly where it's kept, whether that's in the main medical emergency equipment dental practice bag or a dedicated clinical fridge.
What happens if our emergency equipment is found to be expired during a CQC inspection?
Discovering expired equipment during an inspection usually results in a breach of CQC Regulation 12 regarding safe care and treatment. This failure can negatively impact your practice's "Safe" and "Well-led" ratings. Inspectors view expired drugs or uncharged equipment as a sign of poor clinical governance and a risk to patient safety. You'll likely be issued a Requirement Notice, necessitating a formal action plan and a follow-up audit to prove the issue has been resolved.