Syncope Management for Dental Teams: A Comprehensive Training Guide for 2026

Did you know that vasovagal syncope accounts for over 60% of all reported medical emergencies in the dental surgery? With nearly half of all practitioners managing at least one collapse annually, the need for robust syncope management dental training has never been more critical for patient safety. It's entirely natural to feel a sense of pressure when a patient suddenly loses consciousness, especially when you must quickly distinguish a simple faint from a more serious cardiac event.
We understand that keeping a team organised during a crisis is often the biggest challenge. This guide provides the clear, functional protocols you need to lead a coordinated response with confidence. You'll master the ABCDE approach and learn how to implement preventive strategies that stop emergencies before they start. We will preview the latest 2026 GDC-compliant training methods to ensure your practice remains a safe, professional environment for every patient who walks through the door.
Key Takeaways
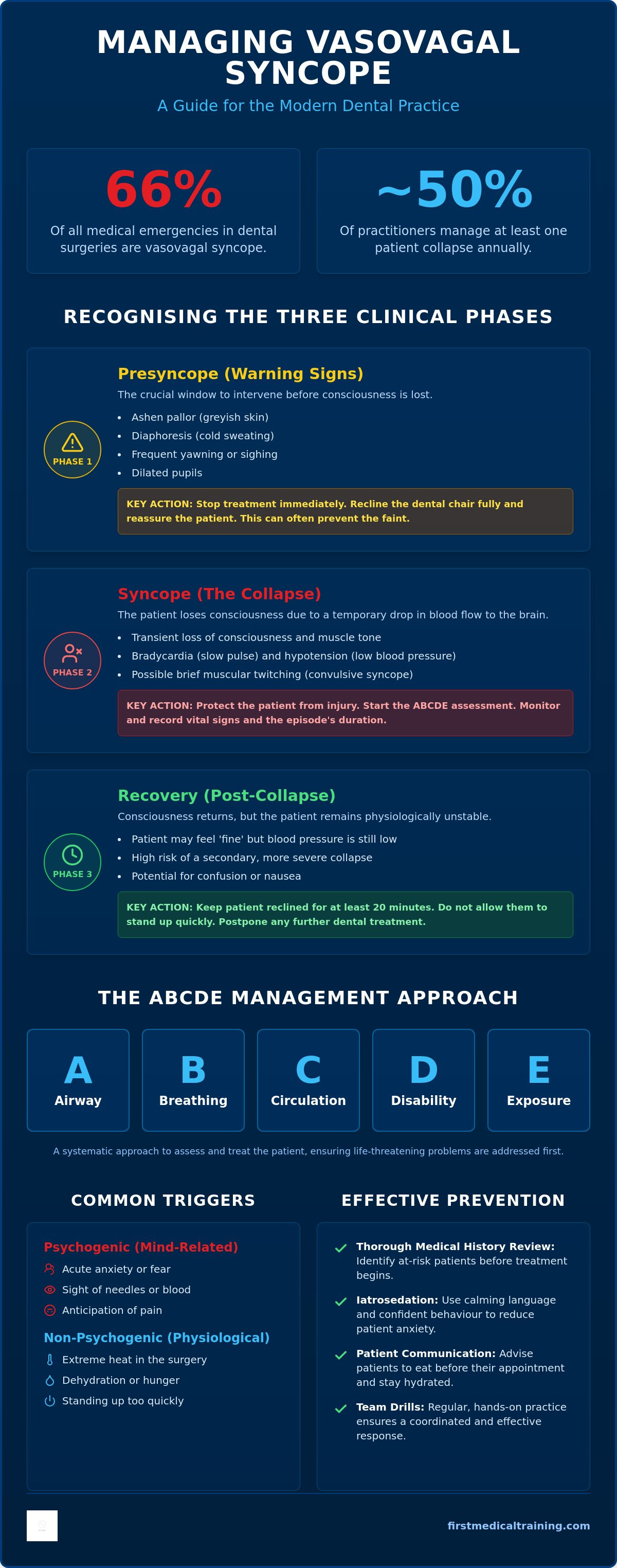
- Learn to recognise the three distinct clinical phases of vasovagal syncope, allowing you to intervene during presyncope before a complete loss of consciousness occurs.
- Master the P-CAB-D protocol and the ABCDE approach to ensure you can correctly position patients and manage their airway with clinical precision.
- Discover how comprehensive syncope management dental training helps your team meet GDC verifiable CPD requirements whilst improving safety through practical, hands-on drills.
- Implement effective preventive strategies, such as iatrosedation and thorough medical history reviews, to significantly reduce patient anxiety and the risk of collapse.
- Gain the confidence to lead a coordinated team response, ensuring every staff member understands their role during a medical emergency in the surgery.
Understanding Syncope in the Dental Surgery: Why Training Matters
Vasovagal syncope is defined as a transient loss of consciousness resulting from global cerebral ischaemia. Within the dental surgery, it remains the most frequent medical emergency, representing approximately 66% of all reported incidents. This high frequency highlights why robust syncope management dental training is the foundation of any practice's emergency preparedness plan. Beyond the immediate clinical risk, a patient collapse carries a significant psychological weight. A poorly managed event can leave patients feeling vulnerable and may lead to a lasting fear of dental treatment, whilst a professional, confident response reinforces your practice's reputation as a safe and reliable clinical environment.
For a comprehensive overview of syncope, it's helpful to view the condition not as an isolated incident, but as the starting point of a "Chain of Survival" tailored to the dental setting. The professional reputation of your surgery is built on trust. When a crisis occurs, the team's ability to remain calm and methodical acts as a reassuring signal to both the patient and any onlookers. The Chain of Survival in dentistry starts with pre-treatment assessment and ends only when the patient is safely discharged or transferred to secondary care.
The Physiology of a Faint
The vasovagal response is a complex interaction within the autonomic nervous system. It typically begins with an initial adrenergic surge, often referred to as the "fight or flight" response, where the heart rate and blood pressure increase. However, this is rapidly followed by a profound cholinergic response. This sudden shift causes bradycardia and systemic vasodilation, which leads to a rapid drop in blood pressure. During the cholinergic phase, blood pools in the lower extremities, further reducing the volume of blood returning to the heart. Cerebral perfusion pressure is the net pressure gradient that drives oxygen delivery to cerebral tissue; a significant drop in this pressure leads directly to the loss of consciousness observed during syncope.
Common Triggers in the Dental Chair
Triggers in the dental surgery are broadly classified as psychogenic or non-psychogenic. Psychogenic causes are the most common and include acute anxiety, the sight of needles, or the anticipation of pain. These emotional stressors directly stimulate the vasovagal reflex. Non-psychogenic factors are often environmental or physiological, such as extreme heat in the surgery, dehydration, or a patient standing too quickly after a long procedure. Patients who have skipped a meal before their appointment are particularly susceptible, as hypoglycaemia can exacerbate the physiological response to stress. Recognising these triggers is the first step in effective syncope management dental training, as it allows the team to implement preventive measures before the patient's condition escalates.
Identifying the Three Phases of Vasovagal Syncope
Effective syncope management dental training relies on the team's ability to see a collapse coming. Vasovagal syncope follows a predictable chronological path. By categorising the event into three distinct phases, your team can respond with the methodical precision required to maintain patient safety and clinical control.
Early Warning Signs (Presyncope)
Presyncope is your golden window for intervention. Look for the classic "ashen" pallor, where the skin takes on a greyish hue. This is frequently accompanied by diaphoresis (cold sweating) on the forehead and upper lip. Subtle signs like frequent yawning or dilated pupils are often overlooked but are clear indicators of impending collapse. Actionable tip: Stop all treatment immediately. Reclining the chair and reassuring the patient at this stage can often abort the faint entirely.
The Clinical Presentation of Collapse
If the event progresses to syncope, the patient will lose consciousness and muscle tone. You may observe minor muscular twitching, known as convulsive syncope. It's vital to differentiate this from a true seizure; in a faint, the twitching is brief and occurs after the loss of consciousness. Clinically, the patient will exhibit bradycardia and hypotension. The dental nurse should focus on monitoring and recording the pulse rate and the duration of the episode.
The recovery phase is where secondary risks are highest. A patient may feel "fine" moments after waking, but their blood pressure remains unstable. Standing them up too soon risks a secondary, more severe collapse. They should remain in the surgery for at least 20 minutes and should not undergo further treatment that day. Comprehensive syncope management dental training covers the full spectrum of recovery protocols to prevent these complications.
Always watch for "red flag" symptoms that suggest the event isn't a simple faint. Chest pain, incontinence, or a loss of consciousness lasting longer than two minutes require immediate escalation to emergency services. For a detailed breakdown of these clinical indicators, refer to this guide on emergency syncope management in the dental office. To ensure your staff can distinguish these critical differences, consider reviewing our Medical Emergencies in a Dental Practice Course to practice these scenarios in a controlled environment.
Step-by-Step Syncope Management: The ABCDE Approach
When a patient loses consciousness, the clinical environment must transform from a treatment room into a disciplined emergency response centre. The Resuscitation Council (UK) ABCDE framework serves as the gold standard for this transition, providing a structured sequence that prevents vital steps from being overlooked. First, you must stop all dental treatment and remove any instruments, cotton wool rolls, or materials from the patient's mouth to prevent airway obstruction. The immediate priority is to place the patient in a supine position with their legs elevated. This uses gravity to increase venous return and restore cerebral blood flow, which is the most critical step in any comprehensive guide to syncope management.
The Immediate Team Response
Effective syncope management dental training emphasises that a successful outcome is a team effort rather than a solo performance by the dentist. Whilst the clinician manages the patient's airway and breathing, the dental nurse should immediately retrieve the emergency kit and oxygen cylinder. The receptionist plays a vital role by managing other patients in the waiting area and standing by to call 999 if the patient doesn't regain consciousness within two minutes. Work through the assessment methodically:
- Airway: Ensure the airway is clear using a head tilt and chin lift; use suctioning if there is any fluid or debris.
- Breathing: Look, listen, and feel for normal breathing for up to 10 seconds. If breathing is shallow, administer high-flow oxygen at 15 litres per minute using a non-rebreather mask.
- Circulation: Monitor the pulse rate and skin temperature. Aromatic ammonia spirits may be used as a respiratory stimulant, though they're secondary to basic positioning.
- Disability: Assess the level of consciousness using the AVPU scale (Alert, Voice, Pain, Unresponsive).
- Exposure: Loosen tight clothing around the neck or waist to assist breathing and comfort.
Post-Collapse Care and Discharge
Once the patient regains consciousness, don't rush them out of the chair. They should remain supine until they feel stable, then gradually move to a semi-recumbent position. Administering oral glucose or a sugary drink is sensible if you suspect hypoglycaemia contributed to the event, but only once the patient is fully alert and able to swallow safely. Crucially, your discharge protocol must state that patients shouldn't drive themselves home after a significant episode. Their blood pressure and coordination can remain impaired for some time, making them a risk to themselves and others. For a full breakdown of surgery requirements, teams should review their dental practice emergency preparedness checklist to ensure all equipment is ready for use. This level of preparation is what separates a reactive practice from one that truly masters syncope management dental training.
Preventive Strategies and Risk Assessment
The most effective form of syncope management dental training is learning how to prevent a collapse from occurring in the first place. A proactive approach starts with a meticulous review of the patient's medical history. You should specifically look for any previous history of fainting or "needle phobia", as these are the strongest predictors of future episodes. This preventive mindset is shared by other specialised medical providers, such as DKliniek, who ensure patient safety and comfort during procedures like travel vaccinations where needle anxiety is common. Building rapport through iatrosedation techniques is equally vital; a calm, communicative clinician can significantly lower a patient's baseline anxiety, reducing the likelihood of a massive adrenergic surge.
Clinical adjustments also play a central role. Ensuring profound local anaesthesia is achieved before starting a procedure prevents pain-induced triggers. For severely phobic patients, you might consider inhalation or intravenous sedation as part of a structured treatment plan. Don't overlook the surgery environment itself. A stuffy, overheated room can quickly lead to peripheral vasodilation, making it harder for the body to maintain blood pressure during a stressful moment. Keep the surgery well-ventilated and at a comfortable, cool temperature. Providing patients with the option to explore GLI GLI Teeth Whitening Kit for at-home care can also be a helpful way to reduce the number of stressful visits for purely cosmetic procedures.
Identifying High-Risk Patients
Statistics reveal a curious paradox: the "young, fit male" demographic, specifically those aged 16 to 35, is often at the highest risk for vasovagal syncope in the dental chair. This is frequently because they are more likely to suppress or hide their anxiety until their physiological compensation fails. Conversely, elderly patients on antihypertensive medications are prone to orthostatic hypotension. When treating these patients, avoid moving the dental chair too quickly from a supine to an upright position. For pregnant patients, particularly in the third trimester, use a small wedge under the right hip to prevent supine hypotensive syndrome, which occurs when the gravid uterus compresses the inferior vena cava.
The Role of the Dental Team in Prevention
Prevention is a shared responsibility that begins long before the patient enters the surgery. Use your morning huddle to flag any patients known to be anxious or those undergoing complex procedures. Your receptionist is the first line of defence; they can often spot a patient who looks pale, restless, or overly quiet in the waiting room. It is also essential to ensure that patients attending morning appointments have eaten a light meal, as low blood glucose levels significantly lower the threshold for a syncopal event. To ensure your staff can recognise these subtle warning signs and act decisively, consider enrolling in our Medical Emergencies in a Dental Practice Course to build a truly resilient team.
Syncope Training and GDC CPD Compliance
GDC compliance is far more than a box-ticking exercise; it's a fundamental commitment to patient safety within the clinical environment. For dental professionals in 2026, the General Dental Council (GDC) maintains a clear stance on emergency preparedness. They recommend that all dental professionals complete at least 10 hours of medical emergencies CPD per five-year cycle, with a strong suggestion that at least two of these hours are tackled annually. Whilst theoretical knowledge is important, the GDC emphasises that this training should be as practical as possible. This is where dedicated syncope management dental training provides the most value, moving beyond passive learning to active, life-saving skill acquisition.
First Medical Training structures the Medical Emergencies in a Dental Practice Course to meet these rigorous standards whilst building genuine clinical confidence. A vital part of this compliance involves the meticulous documentation of any incidents. If a patient collapses, the details must be recorded in a dedicated incident log. This log is essential for CQC inspections and GDC audits, as it demonstrates your practice’s ability to reflect on emergency events and refine your protocols. It should include the timeline of the syncope episode, the specific interventions made, and the patient's recovery status before discharge.
Building Clinical Confidence Through Drills
Muscle memory is the most reliable tool a dental team possesses during a crisis. When a patient loses consciousness, you don't want to be searching for a manual; you want your hands to move automatically to the correct positions. Regular in-practice drills allow the team to practice mock syncope scenarios in the actual surgery where they work. This helps identify practical challenges, such as the best way to position the chair in a confined space or who is responsible for retrieving the oxygen. For a deeper look at your professional obligations, review our guide on GDC CPD requirements for medical emergencies.
Choosing the Right Training Provider
Selecting a training provider with specific expertise in the dental sector ensures that the scenarios practiced are relevant to your daily work. Onsite training is particularly effective for whole-team cohesion, as it involves everyone from the principal dentist to the apprentice nurse and the reception team. This collective training ensures that when an emergency occurs, the response is synchronised and calm. When you are ready to refresh your team's skills and ensure your practice remains fully compliant, you can book your next medical emergencies training with First Medical Training to ensure your surgery meets the highest standards of emergency care.
Securing Your Practice's Future Clinical Safety
Mastering the three distinct phases of a faint and the structured ABCDE response framework ensures your team is prepared for the most common medical emergency in the surgery. By shifting from a reactive stance to a preventive one, you protect both your patients' health and your professional reputation. High-quality syncope management dental training is the essential bridge between theoretical GDC guidelines and the calm, life-saving precision required during a real-world collapse.
Our training sessions provide GDC-compliant verifiable CPD and focus on practical, hands-on drills for the whole team. You will learn from expert instructors who bring real-world medical experience directly into your clinical environment. This methodical approach builds the muscle memory necessary to lead a coordinated response with quiet confidence. It's about ensuring every staff member, from the reception desk to the chairside, knows exactly what to do when seconds count.
Book Your Team’s Medical Emergencies Training Now to secure your compliance and take the final step towards total clinical readiness. We look forward to supporting your team as a trusted partner in your professional development.
Frequently Asked Questions
What is the most common cause of syncope in a dental practice?
Psychogenic triggers, specifically acute anxiety and the fear of pain, are the most frequent causes of collapse. These emotional stressors often peak during the administration of a local anaesthetic, which accounts for approximately 75% of reported cases. Effective syncope management dental training teaches teams how to identify these anxious patients early, allowing for preventive measures like iatrosedation to be used before the needle is even presented.
How should I position a pregnant patient who feels faint in the chair?
You must avoid placing a pregnant patient in a completely flat supine position, especially during the third trimester. The weight of the uterus can compress the inferior vena cava, leading to supine hypotensive syndrome. Instead, tilt the patient onto their left side or place a firm wedge under their right hip. This ensures blood flow returns to the heart effectively whilst you manage the airway and monitor their recovery.
Is it necessary to call 999 for a simple vasovagal faint?
In most cases, a simple faint doesn't require an ambulance if the patient regains consciousness within two minutes of being placed in a supine position. However, you must call 999 immediately if the patient remains unconscious after this window or if they exhibit "red flag" symptoms. These include chest pain, a pulse that remains very slow or irregular, or if the collapse was preceded by a seizure or significant trauma.
What emergency drugs are used for syncope management?
Oxygen is the primary "drug" used during a syncopal event, administered at a high flow rate of 15 litres per minute via a non-rebreather mask. Aromatic ammonia spirits can also be used as a respiratory stimulant to help "wake" the patient. Once the patient is fully conscious and able to swallow safely, oral glucose or a sugary drink may be provided if you suspect that low blood sugar contributed to the collapse.
How often does the GDC require medical emergency training for dental staff?
The GDC requires all registered dental professionals to complete at least 10 hours of verifiable CPD in medical emergencies per five-year cycle. It is highly recommended that at least two of these hours are completed annually to ensure skills remain fresh. Participating in regular syncope management dental training as a full team helps meet these standards whilst ensuring that every staff member knows their specific role during a crisis.
Can a patient continue their dental treatment after recovering from syncope?
No, you shouldn't continue dental treatment during the same visit after a patient has lost consciousness. Even if the patient feels better, their cardiovascular system remains unstable and the risk of a secondary, more severe collapse is high. The patient should be observed for at least 20 minutes and then discharged into the care of a responsible adult. They shouldn't drive themselves home after such an episode.
What is the difference between syncope and orthostatic hypotension?
Syncope is a reflex response to a trigger, such as fear or pain, that causes a sudden drop in heart rate and blood pressure. Orthostatic hypotension is a mechanical failure of the body to maintain blood pressure when a patient moves from a lying to a standing position. This is particularly common in elderly patients or those taking antihypertensive medications. Unlike a vasovagal faint, orthostatic hypotension doesn't usually involve a slow heart rate.
Should I use a defibrillator if a patient faints?
You don't need to use an Automated External Defibrillator (AED) for a simple faint where the patient is still breathing and has a pulse. An AED is only used when a patient is in cardiac arrest, meaning they are unresponsive and not breathing normally. If your ABCDE assessment confirms the patient has a clear airway and is breathing, focus on positioning and oxygen. Only deploy the AED if the patient's condition worsens and they stop breathing.