Cardiac Arrest Management in Dental Practice: The 2026 Clinical Standard

If a patient collapsed in your chair tomorrow, would your team move as a single, synchronised unit, or would the next ten minutes be defined by hesitation and uncertainty? It is a scenario every dental professional dreads. Effective cardiac arrest management in dental practice requires more than just ticking a box; it demands a team that understands the latest clinical standards. The pressure to maintain GDC compliance while navigating the nuances between Basic Life Support (BLS) and Immediate Life Support (ILS) can often feel overwhelming, leaving many clinicians worried about how they would actually perform during a real-life crisis.
This guide will help you master the 2026 Resuscitation Council UK protocols and clarify the exact training your surgery needs to remain compliant. We will explore the unified 6-link Chain of Survival, the shift toward ILS as the modern clinical gold standard, and how to turn your GDC verifiable CPD hours into genuine, life-saving confidence. By the end, you will have a clear roadmap for equipment requirements and a well-drilled team ready to act with quiet authority when it matters most.
Key Takeaways
- Align your surgery with the 2026 Resuscitation Council UK protocols to ensure full regulatory compliance and patient safety.
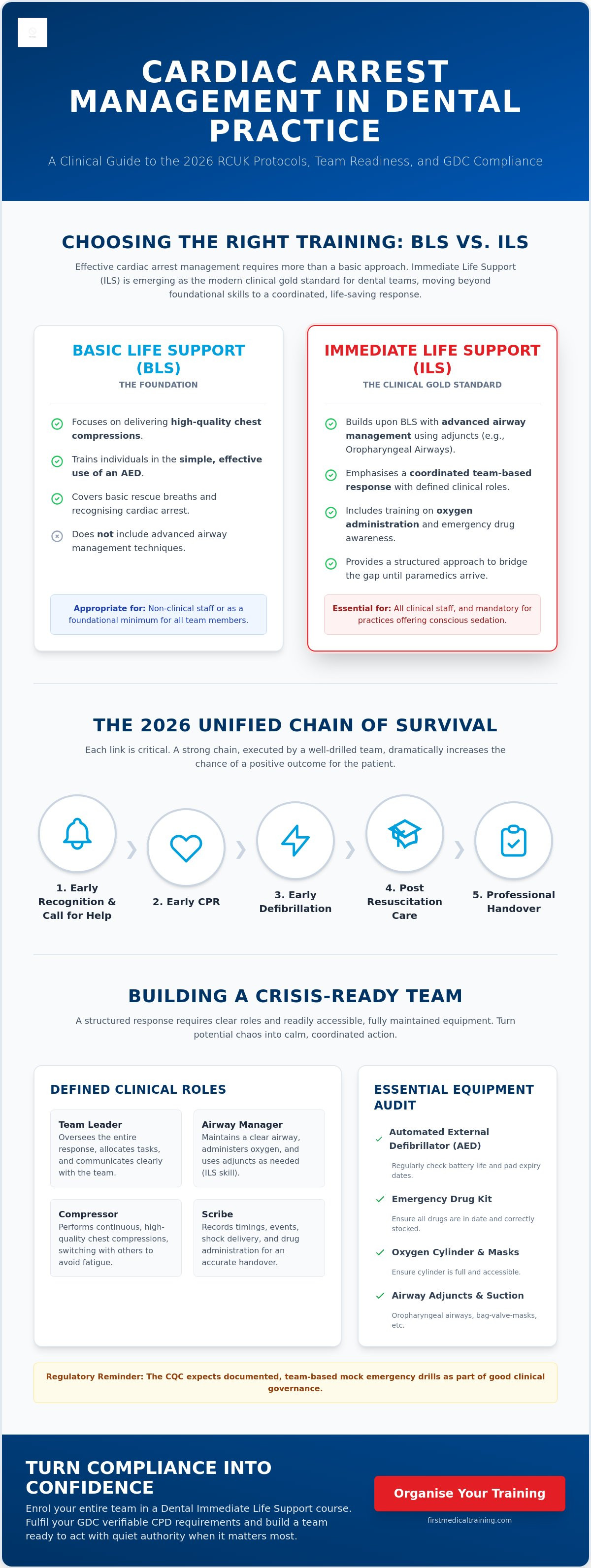
- Distinguish between BLS and ILS training to implement the most appropriate standard of cardiac arrest management in dental practice for your team.
- Learn to execute the updated 2026 resuscitation algorithm, including specific airway management techniques for patients whilst in the dental chair.
- Define clear clinical roles for your staff, such as the Airway Manager and Scribe, to ensure a structured and calm response during a crisis.
- Audit your emergency drug kit and AED readiness against the latest essential equipment checklists required for modern dental surgeries.
Current Standards for Cardiac Arrest Management in Dental Practice
Sudden Cardiac Arrest (SCA) in a clinical dental environment is the abrupt cessation of mechanical heart activity, resulting in the immediate loss of consciousness and breathing. In the surgery, this life-threatening event can be triggered by pre-existing conditions, though it is occasionally exacerbated by acute pain, extreme patient anxiety, or adverse reactions to local anaesthetics. The Resuscitation Council UK (RCUK) provides the authoritative framework for our response. Their 2026 protocols place a renewed emphasis on the chain of survival, which streamlines the transition from initial recognition to advanced care. For the modern dental team, understanding these updates is the foundation of professional competence.
The General Dental Council (GDC) classifies medical emergencies as a "Highly Recommended" topic for verifiable CPD. This mandate requires dental professionals to undertake regular training to ensure their skills remain sharp. Resuscitation techniques are highly perishable; research indicates that the quality of chest compressions and the speed of AED deployment can decline significantly within just a few months of training. This reality has driven a shift in industry expectations. We are moving away from simple Basic Life Support (BLS) toward the more robust standard of Dental Immediate Life Support (ILS) Training. This higher level of preparation ensures that cardiac arrest management in dental practice is treated as a coordinated team intervention rather than a series of isolated individual tasks.
The Legal and Regulatory Framework
Compliance involves more than just attending a lecture. The Care Quality Commission (CQC) expects practices to maintain a fully operational Automated External Defibrillator (AED) and a correctly stocked emergency drug kit. It's vital to have a system for checking expiry dates and battery health. Documented, team-based mock medical emergency drills are now a cornerstone of good clinical governance. These rehearsals allow your staff to familiarise themselves with the layout of the emergency bag and the specific challenges of managing a collapse within the confines of a dental surgery. Evidence of these drills is often a key metric during regulatory inspections.
Duty of Care and Clinical Governance
Your duty of care to the patient remains absolute whilst they are under your roof. This responsibility is particularly acute for practices offering conscious sedation, where the risk of respiratory depression requires a more sophisticated response. Failing to provide adequate resuscitation equipment or failing to train staff to a recognised standard carries significant legal and professional risks. By enrolling the whole team in a Medical Emergencies in a Dental Practice Course, you proactively reduce your clinical risk profile. This structured approach builds a culture of safety that reassures both your patients and your professional indemnity providers.
Dental Immediate Life Support (ILS) vs BLS: Choosing the Right Training
Standard Basic Life Support (BLS) is often the baseline for medical emergency training, but it's rarely enough for a high-stakes clinical environment. Effective cardiac arrest management in dental practice isn't just about individual effort; it's about a coordinated, rapid response that bridges the gap until paramedics arrive. Whilst BLS focuses on high-quality chest compressions and simple AED use, Immediate Life Support (ILS) introduces advanced techniques that can significantly improve patient outcomes during those critical first minutes.
For clinics providing conscious sedation, the choice is already made for you. Regulatory bodies and professional guidelines expect a higher level of intervention because sedation inherently increases the risk of respiratory complications. Prioritising Dental Immediate Life Support (ILS) Training ensures your clinical team can manage airway obstruction and use advanced adjuncts with confidence, moving beyond the limitations of simple rescue breaths.
When is BLS Sufficient?
BLS remains a solid and appropriate standard for non-clinical staff, such as receptionists or administrative teams. It provides them with the essential tools to recognise a collapse and start early CPR without being overwhelmed by technical medical equipment. However, it has clear limitations when dealing with advanced airway obstruction or respiratory arrest. For the wider team, an Emergency First Aid at Work qualification often provides the necessary breadth for non-clinical incidents whilst supporting the core resuscitation effort in a secondary role.
The Advantages of Dental-Specific ILS
The real value of an ILS approach lies in the integration of professional equipment that is already present in your surgery. ILS training focuses on the practical application of these tools in a team-based setting. Key advantages include:
- Airway Management: Using oropharyngeal (OP) airways and Bag-Valve-Mask (BVM) ventilation to maintain a patent airway more effectively than mouth-to-mask methods.
- Oxygen Administration: Understanding how to integrate high-flow oxygen into the resuscitation algorithm to improve myocardial and cerebral oxygenation.
- Advanced AED Use: Developing a deeper understanding of shockable versus non-shockable rhythms, which allows for a more professional handover to the ambulance service.
- Team Leadership: Training clinical staff to take charge of the scene, delegate tasks, and maintain a calm, structured environment.
Assessing your practice needs depends on your patient demographics and the complexity of your procedures. If you treat elderly patients or those with multiple co-morbidities, the likelihood of a cardiac event increases. Modern cardiac arrest management in dental practice relies on this transition from basic skills to integrated life support. You might find that a comprehensive Medical Emergencies in a Dental Practice Course is the most efficient way to align your entire team's skills with these 2026 standards.
The 2026 Algorithm for Resuscitation in the Dental Chair
When a patient loses consciousness, the transition from clinical procedure to emergency response must be instantaneous. The 2026 algorithm prioritises speed and team coordination through a structured sequence of actions. Start with the "Danger, Response, Shout" sequence. Ensure the area is safe, check for a response with a gentle shake and shout, and immediately call for the emergency kit and an AED. If the patient is not breathing normally, or only gasping, you must assume cardiac arrest has occurred. This rapid recognition is the most critical factor in improving survival rates.
Effective cardiac arrest management in dental practice requires a decisive choice regarding the patient's location. Whilst traditional training often suggests moving the patient to the floor, modern dental chairs are designed to go fully flat, providing a stable platform for resuscitation without the delay or risk of injury associated with moving a heavy patient in a confined space. High-quality chest compressions must begin immediately at a ratio of 30 compressions to 2 breaths, maintaining a rate of 100 to 120 beats per minute and a depth of 5 to 6 cm.
Once the AED arrives, it takes priority. Apply the pads whilst compressions continue to minimise "hands-off" time. Follow the voice prompts exactly, ensuring the "Clear" protocol is strictly observed before a shock is delivered. Nobody should touch the patient whilst the AED is analysing or charging. After the shock, or if no shock is advised, resume CPR immediately. When the paramedics arrive, provide a structured handover using the SBAR (Situation, Background, Assessment, Recommendation) framework to ensure a seamless transfer of care.
Managing Collapse in the Dental Chair
The decision to treat in the chair or on the floor depends on your surgery’s layout. If you have sufficient space and a firm floor, moving the patient may be preferable, but for most modern surgeries, the chair is the faster option. Ensure the chair is fully reclined and the headrest is adjusted to maintain an open airway. The optimal position for chest compressions in a dental surgery is with the patient in a fully reclined, flat dental chair adjusted to a height that allows the rescuer to stand with their shoulders directly over the patient’s sternum.
Advanced Airway and Oxygen Protocols
Airway management is more effective when treated as a two-person task. One rescuer maintains the mask seal using the "E-C" grip whilst the second rescuer provides gentle, consistent squeezes of the bag-valve-mask (BVM). Integrating an oropharyngeal airway (OPA) is essential to prevent the tongue from obstructing the posterior pharynx in an unconscious patient. During resuscitation, emergency oxygen should be delivered at a flow rate of 15 litres per minute to maximise the concentration of oxygen in the lungs and circulating blood.
Team Dynamics and Emergency Equipment Requirements
A successful resuscitation attempt depends as much on the organisation of the team as it does on the clinical skills of the individual. In a crisis, the physical environment of a dental surgery can quickly become chaotic without predefined roles. Effective cardiac arrest management in dental practice relies on three core pillars: the Lead Responder, the Airway Manager, and the Scribe. The Lead Responder, typically the dentist, maintains a "global" view of the scene, directing the algorithm and making the final call on drug administration. The Airway Manager focuses exclusively on ventilation and suction, whilst the Scribe provides the vital link between the clinical team and the emergency services, recording the timing of shocks and drugs for the eventual handover.
Your emergency trolley serves as your clinical lifeline. It must be centrally located and easily accessible to all staff members. A standard 2026 checklist includes a functional AED, high-flow oxygen cylinders, portable suction with appropriate catheters, and a GDC-compliant emergency drug kit. Beyond the standard kit, many surgeries now include the LifeVac anti-choking device. This addition is particularly useful in preventing secondary cardiac arrest caused by profound hypoxia during a foreign body airway obstruction. To ensure these tools are ready when needed, your practice should implement a weekly protocol for checking expiry dates and battery status, with a signed log to satisfy CQC requirements.
Building this level of readiness requires more than just reading a manual. To truly prepare your staff, you can book a Medical Emergencies in a Dental Practice Course to run through these dynamics in your own clinical environment.
Effective Communication During a Crisis
Errors in emergency medicine often stem from poor communication rather than a lack of knowledge. Using "Closed-Loop" communication is a simple way to prevent mistakes; when the Lead Responder requests a drug, the person administering it should repeat the command back clearly before confirming once the task is complete. Whilst the clinical team works, reception staff must manage the waiting room. They should clear the corridors, direct the ambulance crew upon arrival, and support other patients who may be distressed. Once the patient is transferred, a post-event debrief is essential. This allows the team to process the psychological impact of the event and identify any areas for improvement in their cardiac arrest management in dental practice protocols.
AED Maintenance and Placement
An AED is only useful if it is functional and easy to find. Standardised green and white signage should be visible from multiple points in the surgery. Ensure that all staff, including locums or temporary nurses, are shown the AED location during their morning induction. Daily checks should confirm the "ready" light is flashing, whilst monthly audits should verify that the adhesive pads are still within their use-by date. If your AED pads are reaching the end of their shelf life, or if you need to upgrade your device, our Automated External Defibrillator (AED) Training Course provides the perfect opportunity to refresh your team's practical skills.
Organising Your Team’s Dental Immediate Life Support Course
Moving from theoretical knowledge to clinical readiness requires a structured approach to training. Whilst reading about the latest protocols is a vital first step, true competence in cardiac arrest management in dental practice is forged through practical, team-based rehearsal. Organising an in-practice course is often superior to sending staff to external training centres. When your team trains together in their own surgery, they aren't just learning skills; they are learning how to navigate their specific clinical environment, where the emergency oxygen is stored, and how to move effectively around their own dental chairs.
A high-quality Medical Emergencies in a Dental Practice Course should provide more than just a certificate. It should offer a comprehensive review of the 2026 RCUK algorithms, hands-on practice with airway adjuncts, and realistic simulations of patient collapse. Before booking, always verify the credentials of your training provider. Ensure their instructors have frontline clinical experience and that the certification is recognised by the GDC. Integrating this training into your annual professional development plan ensures that cardiac arrest management in dental practice remains a sharp, habitual skill rather than a half-remembered theory.
Customising Training to Your Surgery Environment
Our trainers don't just bring generic manikins; they integrate your own equipment into the session. Using your practice's specific AED, suction units, and emergency drug kits ensures that there is no hesitation when a real crisis occurs. We tailor scenarios to match your patient demographic, whether you focus on paediatric care or complex geriatric dentistry. First Medical Training prioritises hands-on simulation over purely theoretical learning because muscle memory is the only reliable tool when high-pressure clinical decisions must be made in seconds. This bespoke approach builds a level of team confidence that external, "one-size-fits-all" courses simply cannot replicate.
Securing Your GDC Verifiable CPD
Maintaining your professional registration requires clear evidence of learning that meets the GDC’s criteria for verifiable CPD. A robust course will provide a clear set of aims and objectives, anticipated learning outcomes, and a certificate that states the number of hours completed. Booking a group session for the entire team is the most efficient way to achieve this, as it minimises practice downtime and ensures everyone receives the same high standard of instruction simultaneously. It’s a pragmatic solution that satisfies both regulatory requirements and your duty of care to your patients. To ensure your surgery is fully prepared for 2026, Book your Dental ILS or Medical Emergencies course with First Medical Training today.
Future-Proofing Your Emergency Response
Mastering cardiac arrest management in dental practice is a continuous journey of professional development rather than a one-off task. By embracing the 2026 RCUK protocols and transitioning toward an Immediate Life Support standard, you provide your patients with the highest possible level of clinical safety. Success in a crisis relies on the seamless integration of high-quality CPR, rapid AED use, and a well-drilled team that understands their specific roles within the surgery environment. Replacing hesitation with a structured, rehearsed response ensures that your surgery remains a safe space for every patient who walks through the door.
Founded in 2006, First Medical Training brings over two decades of specialised dental expertise directly to your clinical setting. Our comprehensive approach includes everything from ILS and Mental Health First Aid to being accredited providers of the LifeVac anti-choking device. We understand the unique pressures of the dental environment and are dedicated to building your team's confidence through practical, hands-on simulation.
Enquire about our Dental Immediate Life Support (ILS) courses for your team today to ensure your practice remains compliant, capable, and ready to act. Your commitment to these standards now ensures you are prepared to save a life when every second counts.
Frequently Asked Questions
Is annual cardiac arrest training a mandatory requirement for UK dentists?
Yes, the General Dental Council (GDC) requires all registered dental professionals to undertake annual verifiable CPD in medical emergencies. This training ensures that your life-saving skills remain sharp and that your practice remains compliant with the latest Resuscitation Council UK guidelines. Maintaining this annual standard is a core component of your professional indemnity and clinical governance requirements.
What is the difference between BLS and Dental Immediate Life Support (ILS)?
Basic Life Support (BLS) focuses on chest compressions and simple AED use, whilst Dental ILS introduces advanced airway management and the use of adjuncts like bag-valve-masks. ILS is specifically designed for clinical environments, allowing teams to manage a collapse more effectively until the ambulance service arrives. It provides a more robust framework for cardiac arrest management in dental practice, particularly for surgeries offering conscious sedation.
Does a dental practice need to have an AED on-site by law in 2026?
Yes, current GDC and CQC standards mandate that every dental practice must have a functional Automated External Defibrillator (AED) on-site. It's no longer acceptable to rely on neighbouring businesses or public access units. Your AED must be checked regularly to ensure the pads and batteries are within their expiry dates and that the device is ready for immediate deployment during a crisis.
Can dental nurses lead the resuscitation attempt in a cardiac arrest scenario?
Dental nurses can and should lead the resuscitation attempt if they are the first person to recognise the patient's collapse. In a well-drilled team, the first responder takes the Lead Responder role regardless of their clinical grade until a more senior clinician can take over. Effective training ensures that every staff member feels empowered to initiate the algorithm and direct the early stages of the rescue.
What emergency drugs must be present in a dental surgery for cardiac arrest management?
The primary drug for cardiac arrest is Adrenaline (1:1000), though this is typically administered by paramedics rather than dental staff during the initial CPR phase. Your emergency kit must also contain Aspirin, Glucagon, Glyceryl Trinitrate (GTN), Midazolam, and Salbutamol. Whilst not all these drugs are for cardiac arrest, they are essential for managing the acute medical emergencies that can often precede a collapse.
How many hours of verifiable CPD does a medical emergencies course provide?
A standard Medical Emergencies in a Dental Practice Course typically provides three to four hours of GDC verifiable CPD. This time is dedicated to both theoretical updates and practical simulations, ensuring you meet the recommended annual requirements. Always check that your training provider issues a certificate that clearly states the learning outcomes and the total duration of the training session.
Should we remove a patient from the dental chair before starting CPR?
You should only move a patient to the floor if the dental chair cannot be reclined fully flat or if there is insufficient space to work around it. Most modern dental chairs provide a stable, firm platform for chest compressions when placed in the emergency position. Moving a patient can waste vital seconds; therefore, treating in the chair is often the fastest option for cardiac arrest management in dental practice.
What is the recommended frequency for practice-based medical emergency drills?
The Resuscitation Council UK recommends that dental teams conduct mock medical emergency drills at least every six months. These sessions allow the team to practice their specific roles and familiarise themselves with the location of equipment without the pressure of a real crisis. Documenting these drills is a key requirement for demonstrating effective clinical governance during a CQC inspection or audit.