Hypoglycaemia Emergency Dental Training: Managing Diabetic Crises in the Chair

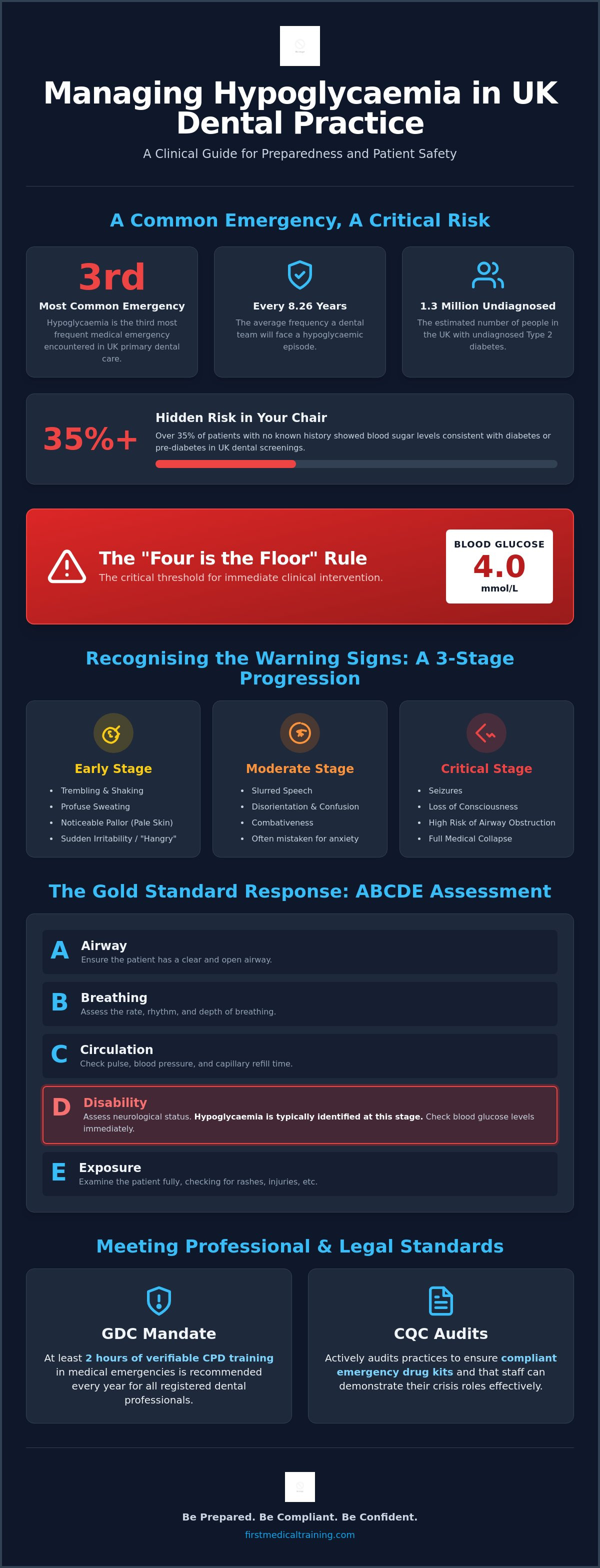
Hypoglycaemia is the third most common medical emergency in UK primary dental care, with dental teams encountering an episode on average every 8.26 years. It's a statistic that underscores why specialised hypoglycaemia emergency dental training is essential for every member of the practice. You likely already know the sinking feeling of checking a medical history and seeing "Type 1 Diabetes," wondering if today is the day a patient collapses in your chair. The pressure to stay current with Resuscitation Council UK standards whilst meeting your annual verifiable CPD requirements can feel overwhelming, especially when you're balancing clinical excellence with patient safety.
This guide will help you master the clinical protocols and equipment requirements needed to manage a diabetic crisis with total composure. You'll learn exactly how to implement the "Four is the Floor" rule for blood glucose readings below 4.0 mmol/L and when to transition from oral glucose to the Glucagon protocol. We will preview the essential team-based response strategies that turn a chaotic emergency into an organised, life-saving drill, ensuring your whole team is prepared to act when seconds count.
Key Takeaways
- Understand why blood glucose levels below 4.0 mmol/L require immediate action and how factors like patient anxiety can trigger a sudden drop.
- Master the ABCDE assessment framework to rapidly distinguish between mild symptoms and a severe hypoglycaemic collapse in the chair.
- Ensure your surgery remains compliant with 2026 standards by maintaining a fully equipped emergency drug kit and a calibrated glucometer.
- See how hypoglycaemia emergency dental training delivered in your own practice environment builds team confidence and clarifies individual roles during a crisis.
- Learn to implement "silent" alarms and organised surgery layouts to facilitate a calm, efficient response from the entire dental team.
Understanding Hypoglycaemia Risks in Modern Dental Practice
Hypoglycaemia occurs when blood glucose levels fall below 4.0 mmol/L, a threshold commonly referred to as the "Four is the Floor" rule in UK dental surgeries. In a clinical setting, this drop in blood sugar is more than a minor complication; it's an acute medical emergency that requires immediate intervention. Whilst many clinicians feel confident in their general skills, the specific nuances of managing Diabetic Hypoglycemia whilst a patient is mid-procedure can be daunting. Comprehensive hypoglycaemia emergency dental training ensures your team can bridge the gap between a routine check-up and a medical crisis with steady, practiced confidence.
The prevalence of diabetes amongst the UK population continues to rise. As of July 2026, data suggests that nearly 1.3 million people may be living with undiagnosed Type 2 diabetes. Recent clinical research conducted in UK dental settings revealed that over 35% of patients without a known history of the condition actually displayed blood sugar levels consistent with diabetes or pre-diabetes during routine screenings. This means every patient who walks into your surgery represents a potential risk, regardless of what their medical history form currently states.
Why Dental Patients Are at Higher Risk
Dental appointments create a perfect storm for glucose instability. Patients often fast before morning appointments to avoid feeling nauseous during treatment, or they may simply miss a meal due to anxiety. This procedure-related stress triggers the release of adrenaline, which can mask early warning signs of a drop in blood sugar. The metabolic demands of the body change under stress, causing glucose to be consumed more rapidly. Identifying high-risk patients during your initial medical history review is essential. You should specifically look for those on insulin or sulphonylureas, as these individuals are most susceptible to sudden, severe episodes whilst in the chair.
The Legal and Regulatory Framework for Training
Maintaining a high standard of emergency preparedness is a non-negotiable legal requirement. The General Dental Council (GDC) mandates that all registered professionals remain competent in managing medical emergencies. This includes a strong recommendation for at least two hours of verifiable training every year. Beyond the GDC, the Care Quality Commission (CQC) actively audits practices to ensure that emergency drug kits are compliant and that staff can demonstrate their roles in a crisis. For a deeper look at these requirements, you can review our gdc cpd requirements medical emergencies guide. Ultimately, hypoglycaemia emergency dental training is the most effective way to meet these professional obligations whilst ensuring the safety of every patient in your care.
Recognising and Responding to Hypoglycaemic Episodes
When a patient begins to deteriorate in the chair, your immediate response must be structured and decisive. The Resuscitation Council UK recommends the ABCDE (Airway, Breathing, Circulation, Disability, Exposure) approach as the gold standard for any clinical crisis. Within this framework, a hypoglycaemic event is typically identified during the "Disability" assessment. Effective hypoglycaemia emergency dental training teaches your team to look past the initial confusion and focus on rapid glucose reversal before the situation escalates to a full collapse.
Clinical Signs and Symptoms to Watch For
Recognising the early onset of a drop in blood sugar is critical for preventing a total loss of consciousness. Patients in the early stages often exhibit trembling, profuse sweating, and noticeable pallor. You might also observe "hangry" behaviour or sudden irritability, which can easily be mistaken for general dental phobia. As the episode progresses to a moderate stage, signs become more neurological. You may notice slurred speech, disorientation, or even combativeness. In a dental setting, these symptoms are frequently misinterpreted as a reaction to local anaesthetics or high levels of anxiety. Without intervention, the patient enters a critical stage characterised by seizures, loss of consciousness, and a high risk of airway obstruction.
The UK Resuscitation Council Protocol for Hypoglycaemia
The management strategy depends entirely on the patient's level of consciousness and their ability to swallow safely. For a conscious patient, the protocol involves administering 10 to 20 grams of a fast-acting carbohydrate. This is typically achieved using glucose tablets or oral glucose gel. Following administration, you must observe the "15-minute rule": wait 15 minutes, re-test the blood glucose level, and repeat the dose if there is no clinical improvement or if the reading remains below 4.0 mmol/L. This structured approach is a core component of our Medical Emergencies in a Dental Practice Course, which provides hands-on practice for these scenarios.
If the patient is unconscious or unable to swallow, oral fluids must never be given due to the risk of aspiration. In these severe cases, the protocol shifts to the administration of Glucagon via intramuscular (IM) injection. The standard adult dose is 1mg, whilst children under 8 years of age (or weighing less than 25kg) require a reduced dose of 500 micrograms. Alongside the injection, high-flow oxygen should be administered at 15 litres per minute using a non-rebreather mask. Reliable Management of Medical Emergencies requires that every team member knows exactly where the Glucagon is stored and how to prepare the injection without delay. Once the patient regains consciousness, they should be given a long-acting carbohydrate, such as a biscuit or a sandwich, to prevent a secondary glucose crash.
Essential Emergency Equipment and Drug Kit Compliance
Clinical knowledge is only as effective as the equipment available to support it. For a dental practice to remain compliant with 2026 standards, the emergency drug kit must be meticulously maintained and immediately accessible. Specialised hypoglycaemia emergency dental training emphasises that having the right tools isn't just a clinical preference; it's a regulatory requirement. Your kit must include 1mg of Glucagon for intramuscular injection, along with at least two forms of fast-acting carbohydrate, such as glucose tablets and oral glucose gel. These should be stored at the chairside or in a clearly marked central location known to every staff member.
An automated blood glucose measurement device, or glucometer, is now a mandatory component of your resuscitation equipment. Relying on clinical signs alone can be misleading, as symptoms of hypoglycaemia often mimic other conditions. A calibrated glucometer allows the team to confirm a "Four is the Floor" reading quickly, ensuring that the correct protocol is initiated without guesswork. Because these devices require test strips that can expire or become damaged by moisture, regular calibration and strip-inventory checks are essential for surgery-wide safety. Understanding the complex link between Diabetes and Oral Health helps clinicians appreciate why these diagnostic tools are so vital during routine procedures.
Glucagon vs. Oral Glucose: When to Use What
The decision to use Glucagon over oral glucose is based entirely on the patient's airway safety and level of consciousness. If a patient is drowsy or unable to swallow, administering oral fluids or gels carries a high risk of aspiration, which can lead to life-threatening respiratory complications. In these instances, the 1mg Glucagon injection is the only safe clinical choice. For a detailed breakdown of all mandatory items, you should refer to our medical emergency equipment dental practice guide, which covers the full 2026 compliance requirements.
Maintaining Your Emergency Medical Kit
Effective kit management requires a structured approach. Glucagon is particularly sensitive to storage conditions and has a relatively short shelf life compared to other emergency drugs, making frequent expiry checks critical. We recommend appointing a designated "Emergency Lead" to oversee these protocols. This individual should be responsible for weekly audits of the kit, ensuring that needles and syringes for Glucagon administration remain sterile and that all seals are intact. These checks should be documented as part of your practice's safety records, providing clear evidence for CQC inspectors that your team is prepared for a crisis. Consistent hypoglycaemia emergency dental training ensures that every team member, from the lead dentist to the newest trainee, knows exactly how to navigate the kit under pressure, often supplemented by a pharmacology review from PharmEDU to deepen their clinical understanding.
Team-Based Response and Crisis Management Training
A medical emergency in a busy dental surgery is never a solo event. Success depends on a coordinated, high-speed drill where every team member knows their position and responsibilities. Whilst clinical knowledge is the foundation of care, the logistics of a crisis are what often determine the outcome. Effective hypoglycaemia emergency dental training transforms a chaotic response into a disciplined, life-saving sequence, ensuring that the patient remains the priority whilst the environment is managed safely.
Communication is the first hurdle in any crisis. Initiating a "silent" alarm or using a pre-agreed code word, such as "Assistance to Surgery One," allows you to alert colleagues without causing unnecessary panic amongst other patients in the waiting room. Once the alarm is raised, the physical environment must be adapted immediately. This involves moving the dental stool, bracket table, and cabinetry to allow for 360-degree access to the patient. If a collapse occurs, the team must have enough space to use the emergency kit and facilitate paramedic intervention without obstruction.
Defining Roles During a Medical Emergency
Clarity in leadership is essential to prevent overlapping tasks or critical delays. The Dentist acts as the clinical lead, staying with the patient to perform the ABCDE assessment and administer the Glucagon or oral glucose. The Dental Nurse serves as the primary support, retrieving the emergency kit and oxygen whilst starting a timer to monitor the 15-minute rule for glucose re-testing. Simultaneously, the Receptionist acts as the bridge to external help. They are responsible for calling 999, providing a concise SBAR (Situation, Background, Assessment, Recommendation) report to the operator, and meeting the paramedics at the practice entrance to guide them to the surgery.
Preventive Measures and Pre-Treatment Screening
The most effective way to manage a hypoglycaemic crisis is to prevent it from occurring. Medical histories should be updated at every single visit, not just on an annual basis. For known diabetic patients, the clinical team should ask three specific questions before starting any procedure: "When did you last eat?", "What was your last blood glucose reading?", and "Have you had any recent hypos?". Scheduling high-risk patients for early morning appointments is a simple but effective strategy to minimise the risks associated with fasting or delayed meals. Regular mock drills are the only way to ensure these protocols and roles become second nature for your staff. Our Medical Emergencies in a Dental Practice Course focuses on these team-based simulations to build genuine, surgery-wide readiness.
Elevating Surgery Standards with Professional Emergency Training
General first aid courses often focus on common workplace incidents like minor burns or falls, but they rarely address the clinical complexities of a patient collapsing whilst reclined in a dental chair. Specialised hypoglycaemia emergency dental training is essential because it places the medical crisis within the unique physical and clinical context of your surgery. When your team trains together in their own environment, they develop a spatial awareness that off-site courses cannot replicate. You learn exactly how to navigate around the dental unit and where your specific emergency drugs are kept, turning abstract theory into a practical, life-saving drill.
Clinical confidence isn't built by reading a protocol; it's forged through hands-on repetition. Handling a Glucagon kit for the first time should never occur during a real-life emergency. Professional training allows every staff member to practice assembling syringes and identifying injection sites in a controlled, supportive atmosphere. This practical exposure replaces the fear of the unknown with a sense of steady reliability. It ensures that if a diabetic patient does experience a crisis, your team's response is automatic and precise. This level of preparedness offers immense peace of mind for the staff and projects an image of professional excellence to your patients.
Why Specialist Dental CPD Matters
The GDC requires all registered dental professionals to maintain their skills in managing medical emergencies. Our training is specifically designed to meet GDC Development Outcome C, which focuses on the maintenance and development of clinical knowledge. By learning from industry veterans who understand the nuances of the dental environment, you gain practical insights that go far beyond basic first aid. These experts understand the specific stressors of the chair, such as how procedure-related anxiety can mask the early signs of a glucose drop. For a comprehensive look at maintaining your surgery's standards, you can read our medical emergencies in dental practice course guide.
Booking Your Medical Emergencies in a Dental Practice Course
The 2026 curriculum at First Medical Training Ltd is meticulously structured to be efficient and high-impact. We prioritise the latest Resuscitation Council UK standards, ensuring your practice remains at the forefront of clinical safety. We specialise in delivering group training sessions that bring your entire staff together, from the front-of-house team to the clinical leads. This unified approach clarifies roles and builds a cohesive response strategy that works for your specific surgery layout. Specialised hypoglycaemia emergency dental training is a vital investment in your team's professional development and your patients' safety. Book your specialised dental emergency training today to ensure your practice is fully prepared for any crisis.
Strengthening Your Practice’s Emergency Preparedness
Managing a diabetic crisis in the chair requires more than just clinical knowledge; it demands a synchronised team effort and a perfectly maintained emergency kit. By mastering the protocols and ABCDE assessment framework discussed throughout this guide, you turn potential panic into a structured medical response. Ensuring your surgery is equipped with calibrated glucometers and in-date Glucagon is a vital step toward total regulatory compliance. However, the most effective tool in your surgery is a team that has practised these scenarios together in their own clinical environment.
Since 2006, First Medical Training Ltd has provided specialised hypoglycaemia emergency dental training delivered by medical experts who understand the daily realities of the dental profession. With 20 years of expertise, we help you meet your GDC-aligned verifiable CPD requirements whilst building genuine clinical confidence amongst your staff. Secure your team’s compliance with our Medical Emergencies in a Dental Practice Course and ensure your practice is ready to act with precision. You already provide exceptional dental care; we provide the training to ensure you can protect your patients in any crisis.
Frequently Asked Questions
How often do dental teams need hypoglycaemia emergency training?
Dental teams should undertake medical emergency training annually. The GDC strongly recommends at least two hours of verifiable CPD in this subject every year to maintain clinical readiness. Regular hypoglycaemia emergency dental training ensures that protocols remain fresh in the mind and that team roles are clearly defined before a real crisis occurs. Consistent practice is the only way to ensure a calm response.
Is Glucagon mandatory in a UK dental emergency drug kit?
Yes, Glucagon is a mandatory component of the standard UK dental emergency drug kit. It's specifically required for the management of severe hypoglycaemic episodes where the patient is unconscious or unable to swallow safely. You must ensure the kit contains the 1mg dose and that it remains within its expiry date. Checking these drugs weekly is a core part of surgery compliance.
What is the correct dosage of Glucagon for a child in a dental emergency?
For children under 8 years of age, or those weighing less than 25kg, the correct dosage is 500 micrograms (0.5mg) administered via intramuscular injection. For children over 8 years old or weighing more than 25kg, the standard adult dose of 1mg should be used. Always confirm the patient's age and approximate weight during the initial medical history review to avoid delays.
Can a dental nurse administer glucose gel if the patient is conscious?
A dental nurse can administer oral glucose gel to a conscious patient as part of an established emergency protocol or under the dentist's direction. Nurses play a vital role in the first-line response. Their training includes recognising early symptoms and providing rapid glucose reversal whilst the dentist performs the ABCDE assessment. This collaborative approach ensures the patient receives treatment as quickly as possible.
What should we do if a patient’s blood sugar doesn’t rise after 15 minutes?
If the blood glucose level remains below 4.0 mmol/L after 15 minutes, you should administer a second dose of 10 to 20 grams of fast-acting carbohydrate. If the patient's condition doesn't improve after this second dose, or if they become drowsy and unable to swallow, you must immediately escalate the response and call 999. Never wait for a third reading before seeking help.
How do we record a hypoglycaemic event in the patient’s clinical notes?
You must record a detailed chronological account of the event in the clinical notes. Include the time symptoms started, all blood glucose readings, the specific treatment given, and the patient's recovery time. If 999 was called, record the time of the call and the arrival of the paramedics. Accurate documentation is essential for both clinical continuity and legal protection for the practice.
Should we call 999 for every hypoglycaemic episode in the surgery?
No, 999 is not required for every episode. If a patient is conscious and recovers fully after oral glucose, an ambulance is usually unnecessary. However, you must call for emergency assistance if the patient loses consciousness, suffers a seizure, or fails to respond to two doses of glucose. When you're in doubt, always prioritise patient safety and call for professional medical help.
What is the difference between a hypo and a hyper in the dental chair?
Hypoglycaemia (a "hypo") is low blood sugar that constitutes an immediate clinical emergency. Hyperglycaemia (a "hyper") is high blood sugar that typically develops slowly over several days. Whilst "hypers" are serious, they rarely cause a sudden collapse during a dental appointment. Comprehensive hypoglycaemia emergency dental training focuses on the "hypo" because of its acute, life-threatening nature and the need for rapid intervention.