Cardiac Arrest Response: The 2026 Comprehensive Guide for the Dental Team

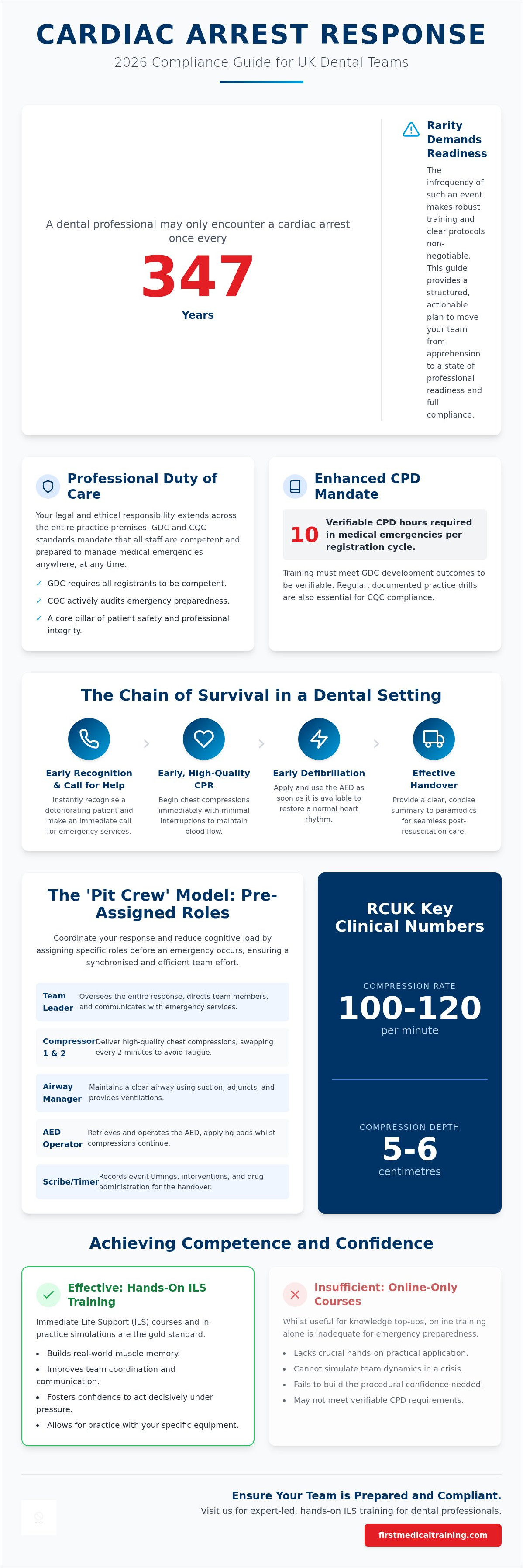
A dental professional might only encounter a cardiac arrest once every 347 years, yet the gravity of those few minutes demands absolute precision. It's understandable if the thought of a real emergency triggers anxiety or if you're worried about "freezing" when the alarm sounds. Navigating the nuances between Basic Life Support (BLS) and Immediate Life Support (ILS) whilst keeping track of expiring equipment can feel like a constant administrative burden. This guide simplifies the cardiac arrest response dental team requirements for 2026, ensuring your practice remains fully compliant with both Resuscitation Council UK and GDC standards.
We recognise that clinical excellence is only half the battle; the other half is the confidence to lead under pressure. We promise to replace confusion with a structured, actionable plan that empowers every member of your staff to act with certainty. You'll gain a clear understanding of the "pit crew" model for role allocation, alongside a breakdown of the mandatory 10-hour CPD requirements. We also provide a pragmatic framework for managing your emergency drugs kit and AED maintenance, moving your team from a state of apprehension to one of professional readiness.
Key Takeaways
- Understand the 2026 RCUK algorithm and your professional duty to provide life-saving care anywhere within the practice premises.
- Learn how to implement the "pit crew" model to coordinate your cardiac arrest response dental team, reducing cognitive load through pre-assigned roles.
- Identify the essential 2026 equipment and medication standards required to ensure your practice remains fully compliant with GDC regulations.
- Discover why hands-on Immediate Life Support (ILS) training and in-practice simulations are more effective than online courses for building real-world confidence.
- Master practical airway management techniques, including the use of adjuncts and suction, to maintain patient stability during a crisis.
The Dental Team’s Duty of Care in Cardiac Arrest Response
Every dental professional holds a profound ethical and legal responsibility to protect their patients. This duty of care isn't confined to the clinical chair. It extends across every square inch of the practice premises. A patient or visitor might collapse in the waiting room, the hallway, or even the staff area. Because of this "anywhere, anytime" reality, the GDC is explicit: all registrants must be competent in managing medical emergencies. The Care Quality Commission (CQC) reinforces this by auditing your practice's emergency preparedness. They expect to see evidence that your team is equipped, trained, and ready to act. A robust cardiac arrest response dental team isn't just a regulatory requirement; it's a fundamental pillar of patient safety and professional integrity. If a patient collapses, they trust that the professionals around them have the skills to intervene effectively.
GDC Standards and Enhanced CPD Requirements
Medical emergencies are a core CPD topic. Under the Enhanced CPD scheme, dental professionals must complete at least 10 hours of verifiable CPD in this area during each registration cycle. To be verifiable, this training must meet the GDC's development outcomes. These outcomes ensure that training improves your clinical practice, team communication, and the overall quality of patient care. The GDC's development outcomes are structured to cover all aspects of professional life:
- Outcome A: Effective communication with patients and the dental team.
- Outcome B: Effective management of self and others.
- Outcome C: Maintenance and development of knowledge within your clinical field.
- Outcome D: Maintenance of skills and behaviours that maintain public confidence.
It's not enough to simply attend a lecture. You must be able to demonstrate learning and reflection. Clinical governance also requires you to document practice-based drills regularly. These simulations ensure that if a crisis occurs, the team's response is instinctive and coordinated. Recording these drills provides the tangible evidence needed for CQC inspections, proving that your preparedness is an active, ongoing process rather than a once-a-year checkbox.
The Chain of Survival in a Dental Setting
The Chain of Survival provides the framework for a successful intervention. It begins with early recognition of the deteriorating patient and an immediate call for help. Once a collapse is identified, the focus shifts to high-quality Cardiopulmonary resuscitation (CPR) and early defibrillation. These are the primary clinical interventions your team will perform. Every second counts whilst waiting for the ambulance service. Your training ensures a seamless transition of care once paramedics arrive. You'll provide them with accurate observations and a clear history of the event, which is vital for the patient's long-term prognosis. A well-drilled cardiac arrest response dental team effectively bridges the gap between the initial collapse and professional emergency care, significantly increasing the chances of a positive outcome.
Clinical Protocols for Resuscitation in Primary Dental Care
The 2026 RCUK algorithm provides a clear, clinical roadmap for the dental surgery. When a patient collapses, the immediate priority is a rapid assessment. Check for a response and look for normal breathing. If the patient is unresponsive and not breathing normally, your cardiac arrest response dental team must initiate the protocol without delay. High-quality chest compressions are the engine of resuscitation. You must aim for a depth of 5 to 6 cm and a rate of 100 to 120 compressions per minute. Minimising interruptions is vital. Every time you stop compressions, the coronary perfusion pressure drops significantly, reducing the chances of a successful outcome.
Airway management in the surgery involves specific tools and techniques. Use high-volume suction to clear any fluid, blood, or debris from the oral cavity. The head-tilt and chin-lift manoeuvre remains the standard for opening the airway; however, the use of oropharyngeal (OP) airways or pocket masks is expected in a professional setting. Integrating the Automated External Defibrillator (AED) should happen as soon as the device arrives. Modern AEDs provide verbal prompts, but the team should be trained to apply pads whilst compressions continue. This ensures the first shock is delivered within seconds of the device becoming available.
Resuscitation in the Dental Chair vs. Floor
The debate over whether to move a patient to the floor is a common concern. Current guidance suggests that if the patient is already in the dental chair, it's often safer and more efficient to perform CPR there. Modern chairs can be lowered to a flat, firm position. Removing the headrest allows for better airway access and a more stable surface. Moving a patient to the floor in a cramped surgery can waste precious time and increase the risk of injury to staff. Ensure the chair is at a height that allows the compressor to lock their elbows and use their body weight effectively.
Immediate Life Support (ILS) vs. Basic Life Support (BLS)
Whilst BLS provides the foundation, Dental Immediate Life Support (ILS) Training is the gold standard for clinical teams. ILS goes beyond simple chest compressions. It incorporates the use of airway adjuncts, emergency oxygen, and a more sophisticated approach to the ABCDE assessment. Transitioning your team from BLS to ILS ensures everyone is comfortable using the specific emergency equipment found in a dental surgery. Practising these advanced skills through a tailored Medical Emergencies in a Dental Practice Course builds the muscle memory needed to act decisively when it matters most. This level of training bridges the gap between basic first aid and the advanced care provided by the ambulance service.
Implementing the Pit Crew Model: Team Roles During a Crisis
Resuscitation in a dental practice is often chaotic because it's such a rare event. The "Pit Crew" model, borrowed from high-performance motorsports, transforms this chaos into a coordinated sequence of events. Instead of everyone rushing to the patient at once, each member of the cardiac arrest response dental team has a specific, pre-defined station. This structure prevents cognitive overload, which is the primary cause of "freezing" during a crisis. When you know exactly where to stand and what to touch, your brain can focus on the technical skill rather than the surrounding noise. Success in these high-stakes minutes depends on the orchestration of the team rather than the heroics of an individual.
Effective response doesn't start when the patient collapses; it starts at the beginning of the clinical day. Use your morning huddle to assign roles based on the day's staffing levels. If a nurse is on lunch or a clinician is running late, the team must know who's covering which station. This proactive organisation ensures that when the emergency alarm sounds, every person moves with purpose. During the event, the team should use closed-loop communication. When the leader gives an instruction, the recipient repeats it back to confirm they've heard it, and then confirms again once the task is complete. This cycle ensures no critical action, like calling 999 or applying AED pads, is left to chance.
The most senior clinician should ideally act as the team leader. Their primary job is oversight, not physical intervention. They shouldn't be performing compressions if other staff are available. Instead, they stand back to monitor the quality of CPR, track the two-minute cycles for shocks, and prepare the clinical handover for the arrival of the paramedics. This "helicopter view" allows the leader to spot errors in technique or equipment failure that those in the thick of the action might miss.
Clinical Roles: Airway, Compressions, and AED
- Role 1 (The Airway): Positioned at the head of the patient. This person is responsible for managing oxygen, using suction to clear the oral cavity, and maintaining an open airway with adjuncts.
- Role 2 (The Compressor): Delivers high-quality chest compressions. This is physically exhausting; the compressor must rotate with another team member every two minutes to ensure the depth and rate remain effective.
- Role 3 (The Equipment Manager): Fetches the AED and the emergency drug kit. They're responsible for switching on the AED and preparing the pads for the compressor to apply.
The Critical Role of the Dental Receptionist
The receptionist is the team's lifeline to external help. Their first priority is calling 999; they must state "Cardiac Arrest" clearly to ensure the call is prioritised as a Category 1 emergency. Beyond the phone call, they manage the practice environment by clearing the waiting room and reassuring other patients to maintain privacy and calm. Finally, they must meet the ambulance at the entrance, ensuring all doors are propped open and having the patient’s medical history and current drug list ready for the paramedics. This coordination ensures that when help arrives, there are no delays in reaching the patient.
Essential Resuscitation Equipment and Medication Standards
Having the right kit is only half the battle; ensuring it works when you need it most is what defines a truly prepared cardiac arrest response dental team. The RCUK minimum equipment list for 2026 remains the benchmark for clinical compliance. This list isn't a suggestion; it's a requirement for every primary care setting. Your weekly routines must include checking the AED status indicator and verifying the expiry dates on both adult and paediatric pads. If your AED battery is low, the device might fail to charge during a rescue, leading to catastrophic delays. Similarly, expired pads may not adhere correctly to the patient's chest, preventing the device from analysing the heart rhythm accurately.
Oxygen management is another critical area where precision is required. Your practice must stock at least two portable oxygen cylinders, typically size CD, to ensure a continuous supply whilst waiting for the ambulance. These should be set to a flow rate of 15 litres per minute and delivered via a non-rebreather mask with an integral reservoir bag. This setup ensures the patient receives the highest possible concentration of oxygen. Whilst most cardiac arrests in the surgery are primary cardiac events, Adrenaline 1:1000 remains a vital component of your emergency drug kit. It is the priority intervention for arrests secondary to severe anaphylaxis, and its presence is a non-negotiable standard set by the British National Formulary (BNF).
Suction and Airway Management Tools
Portable suction is essential. Relying solely on chair-side suction is a significant risk, as it may fail during a power cut or be physically unreachable if the patient is positioned on the surgery floor. Your portable unit must be battery-operated and capable of generating high-vacuum pressure to clear the airway of vomit or blood. Alongside suction, oropharyngeal (Guedel) airways are necessary to prevent the tongue from obstructing the airway in an unconscious patient. Selecting the correct size is vital; a Guedel that is too large can cause trauma, whilst one that is too small may push the tongue further back. To ensure your equipment checks meet the latest regulatory standards, consider refreshing your knowledge with our Medical Emergencies in a Dental Practice Course.
Anti-Choking Devices in the Dental Setting
A "silent choke" is particularly dangerous in a dental environment. It occurs when a complete obstruction prevents any air movement, meaning the patient cannot cough, speak, or breathe. This rapid hypoxia can lead to a cardiac arrest within minutes. If back blows and abdominal thrusts fail and the patient collapses, the team must transition immediately to the CPR protocol. Integrating the LifeVac anti-choking device into your practice's safety protocol provides an additional, non-invasive layer of protection. This device is especially useful for patients in the dental chair where traditional manoeuvres might be difficult to perform effectively. Once the obstruction is cleared, you must still assess the patient for signs of life and be prepared to initiate full resuscitation if they remain unresponsive.
Achieving Compliance and Confidence Through Dental ILS Training
Compliance is often viewed as an administrative hurdle, but in the context of life-saving care, it represents the minimum standard for patient safety. Whilst online "tick-box" exercises might satisfy the basic requirement for verifiable hours, they cannot replicate the physical and psychological demands of a real-world emergency. Annual, in-practice training is essential for a high-performing cardiac arrest response dental team. It moves beyond theory, allowing staff to handle real equipment and work through scenarios in the actual rooms where they treat patients. This familiarity is vital; knowing exactly where the oxygen cylinder is stored or how to position the AED in your specific surgery layout saves precious seconds when the clock is ticking.
High-fidelity simulation also builds psychological resilience. In a real crisis, the "startle response" can cause even experienced clinicians to hesitate. By practising realistic drills, you desensitise the team to the initial shock of a collapse, allowing muscle memory and protocol to take over. This practical approach ensures that the "Pit Crew" roles discussed earlier become second nature. Integrating Medical Emergencies in a Dental Practice into your annual CPD calendar ensures that your team’s skills remain sharp and that your practice stays ahead of evolving RCUK guidelines.
Choosing a Training Provider: What to Look For
Not all training is created equal. When selecting a provider, look for accreditation and specific expertise in the dental sector. A trainer who understands the unique constraints of a dental surgery, such as managing a patient in a chair or handling high-volume suction, is far more valuable than a general first aid instructor. Post-course support is another hallmark of a quality provider. They should assist with equipment audits and provide clear compliance documentation for your clinical governance folders. Tailored content is a GDC requirement; "one size fits all" training often misses the nuances of dental-specific medical emergencies.
The First Medical Training Approach
At First Medical Training, we have a 20-year history of empowering dental teams across the UK. We understand that clinical confidence is built through practice, not just observation. Our Dental Immediate Life Support (ILS) Training is delivered directly at your practice, ensuring the scenarios we run are completely relevant to your environment. We focus on the human element of care, ensuring your cardiac arrest response dental team is not just meeting a regulatory requirement but is genuinely capable of saving a life. Our goal is to leave your team feeling calm, organised, and ready to lead in any crisis.
Preparing Your Team for Professional Readiness
Mastering a successful cardiac arrest response dental team protocol requires moving beyond basic compliance and embracing a culture of active preparedness. By implementing the pit crew model and maintaining rigorous equipment standards, you ensure that every team member knows their station and their responsibilities. High-fidelity simulations in your own surgery are the most effective way to bridge the gap between theoretical knowledge and clinical confidence, effectively reducing the startle response during a real emergency. This structured approach transforms a high-pressure crisis into a manageable sequence of professional actions.
With over 18 years of specialised dental emergency expertise, we provide accredited 2026 compliant training that meets the highest GDC and RCUK standards. Our national UK coverage allows us to deliver hands-on education directly to your surgery, ensuring your specific environment is ready for any crisis. Book your practice-based Dental Immediate Life Support (ILS) training today to empower your staff and protect your patients. You've worked hard to build a safe clinical environment; we're here to help you maintain it with quiet confidence and professional excellence.
Frequently Asked Questions
How often does a dental team need to undergo cardiac arrest response training?
Dental teams should undergo medical emergency and resuscitation training at least once a year. The General Dental Council (GDC) expects all registrants to keep their skills up to date; annual practice-based sessions are the industry standard for maintaining clinical competence. This ensures that every member of the cardiac arrest response dental team remains familiar with the latest 2026 protocols and equipment. Regular training sessions also help to keep your verifiable CPD hours on track throughout your registration cycle.
Is an AED a legal requirement for a UK dental practice in 2026?
Yes, an Automated External Defibrillator (AED) is a mandatory requirement for all UK dental practices in 2026. The Resuscitation Council UK (RCUK) standards specify that clinical areas must have immediate access to a defibrillator. This device is the only effective treatment for a shockable heart rhythm. Its presence is a critical component of your practice's emergency preparedness and is a key focus during CQC inspections to ensure patient safety.
Can a dental receptionist perform CPR and use an AED?
Every member of the dental team, including receptionists and administrative staff, should be trained in CPR and AED use. In a crisis, the receptionist is often the first person to call 999 and may need to assist with chest compressions or equipment management if clinical staff are occupied. Training the whole team ensures a seamless, coordinated response regardless of who is closest to the patient when they collapse.
What is the most common cause of cardiac arrest in a dental surgery?
Most cardiac arrests are caused by a sudden arrhythmia, such as ventricular fibrillation, where the heart's electrical system malfunctions. Whilst cardiac arrest is extremely rare in the dental surgery, with an estimated incidence of 0.0029 cases per dentist per year, it can also be triggered by severe respiratory failure or anaphylaxis. Recognising a deteriorating patient early through an ABCDE assessment can often prevent a collapse from progressing to a full arrest.
Do we need to move the patient to the floor to perform CPR?
You don't always need to move the patient to the floor. If the dental chair can be lowered to a flat, horizontal position and provides a firm enough surface, it's often safer to perform CPR there. Moving a patient to the floor can be time-consuming and risks injury to the staff in a cramped surgery. However, if the chair's design prevents effective, deep compressions, the floor becomes the necessary alternative for resuscitation.
What emergency drugs should be available for a cardiac arrest?
For a primary cardiac arrest, the most important interventions are high-flow oxygen and the delivery of a shock via an AED. Adrenaline 1:1000 must be available if the arrest is suspected to be caused by severe anaphylaxis. Other emergency drugs in your kit, such as Salbutamol or Glucagon, are used for non-arrest emergencies. Your cardiac arrest response dental team must be familiar with the location and administration of these drugs as specified in the BNF.
How do we record a medical emergency for GDC compliance?
You must record every medical emergency in the patient's clinical notes and complete a formal practice incident report. For GDC compliance, it's also vital to document the team's subsequent debrief and any reflective learning that took place. This evidence demonstrates that your practice follows robust clinical governance procedures. It proves you use real-world events to improve future patient safety and maintain high professional standards.
What is the difference between BLS and ILS for dental professionals?
Basic Life Support (BLS) focuses on chest compressions, rescue breaths, and using an AED. Immediate Life Support (ILS) is a more advanced protocol that includes the use of airway adjuncts, suction, and emergency oxygen. ILS is the recommended standard for dental professionals because it covers the specific equipment found in a surgery. It provides the team with the skills needed to manage a patient more effectively until the ambulance service arrives.