Managing a Hypoglycaemic Emergency in Dental Practice: The 2026 UK Protocol

Your Tuesday morning check-up is proceeding normally until your patient suddenly becomes pale, sweaty, and confused. In a small surgery, the transition from a routine procedure to a life-threatening hypoglycaemic emergency in dental practice happens in seconds. It's a high-pressure moment that tests even the most experienced clinicians. We understand the stress of managing a medical crisis whilst trying to remember precise drug dosages and GDC-compliant protocols under intense pressure.
This guide provides a definitive roadmap for your entire team, fully aligned with the latest 2026 Resuscitation Council UK standards. You'll gain the clarity needed to act decisively, ensuring your practice remains a safe and professional environment for every patient. We'll walk through the updated ABCDE assessment, the exact administration of oral glucose and Glucagon, and the essential steps to satisfy your annual verifiable CPD requirements. By the end of this article, you'll have a clear, step-by-step algorithm that turns clinical anxiety into calm, competent action.
Key Takeaways
- Recognise the clinical threshold for a hypoglycaemic emergency in dental practice and understand how factors like missed meals or insulin imbalances trigger sudden crises.
- Master the systematic ABCDE approach to stabilise patients effectively, prioritising airway patency and safety if a patient's level of consciousness begins to drop.
- Learn the precise protocols for administering oral glucose to conscious patients and the correct transition to intramuscular Glucagon for those unable to swallow.
- Establish clear role allocation within your dental team to ensure a calm, co-ordinated response led by the "Captain of the Ship" management principle.
- Maintain GDC compliance and build long-term clinical confidence through annual verifiable training and the regular implementation of in-surgery mock drills.
What is a Hypoglycaemic Emergency in a Dental Context?
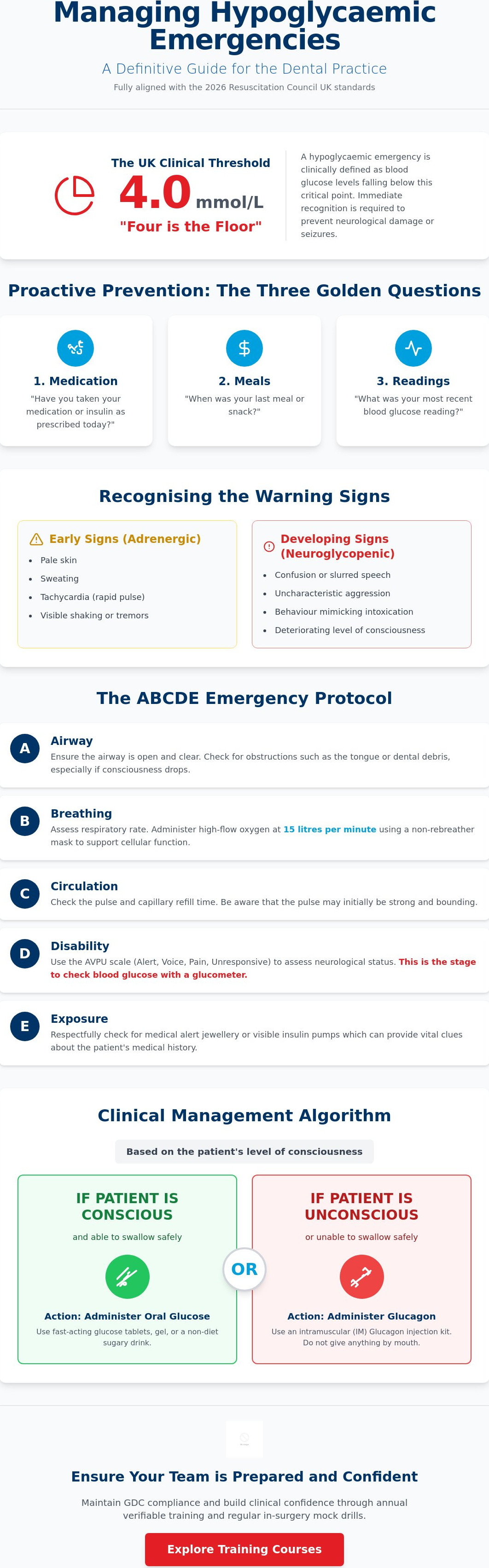
In the UK, a hypoglycaemic emergency in dental practice is clinically defined as blood glucose levels falling below 4.0 mmol/L. While US-based resources often use different metrics, the "Four is the Floor" rule remains the gold standard for British dentistry. This rapid drop in blood sugar occurs when there's a significant mismatch between circulating insulin and available glucose. Common triggers in the surgery include a patient missing a meal before an appointment, over-exerting themselves, or accidentally taking an incorrect insulin dosage. It's a high-stakes situation that requires immediate recognition to prevent a total collapse.
The brain depends entirely on a constant supply of glucose to function. When levels plummet, the patient enters a state of neuroglycopenia. This energy deficit in the brain is the primary risk during dental treatment, as it can lead to permanent neurological damage or seizures if not reversed quickly. You should pay particular attention to "brittle" diabetics or those with historically poor glycaemic control. These individuals are significantly more prone to sudden, severe drops. Understanding What is Hypoglycemia? provides the foundational knowledge your team needs to protect these vulnerable patients.
Recognising the Early Warning Signs
Early detection is vital. Adrenergic symptoms often appear first as the body releases adrenaline to counter the low sugar. You'll notice the patient becoming pale, sweaty, and tachycardic, often accompanied by visible shaking. If the level continues to fall, neuroglycopenic signs emerge. These include confusion, slurred speech, aggression, or behaviour that mimics intoxication. It's easy to mistake these signs for simple dental anxiety or syncope. However, whilst a fainting patient usually recovers quickly once supine, a patient in a "hypo" will continue to deteriorate until glucose is administered. If you're in doubt, always treat for hypoglycaemia; it's the safer clinical path.
Prevention Strategies for the Dental Team
Prevention starts at the front desk and continues through a robust medical history for every patient. Try to schedule diabetic patients for early morning slots. This ensures they've had breakfast and reduces the risk of lunch-time delays causing a crisis. Your reception and clinical staff should always ask the "three golden questions" upon arrival:
- Medication: Have you taken your medication or insulin as prescribed today?
- Meals: When was your last meal or snack?
- Readings: What was your most recent blood glucose reading?
These simple checks create a safety net that prevents most emergencies before the patient even sits in the chair. It's about being proactive rather than reactive, ensuring that your team is always one step ahead of a potential crisis.
To support patients in maintaining their overall health and preventing metabolic emergencies, you might suggest they explore Private GP Consultation (15 Minutes) with the team at Ready Health.
The ABCDE Protocol for Hypoglycaemia Management
The Resuscitation Council UK identifies the ABCDE approach as the definitive framework for managing any medical crisis. When facing a hypoglycaemic emergency in dental practice, this systematic assessment prevents the team from becoming overwhelmed by clinical "tunnel vision". By following a structured sequence, you ensure that life-threatening issues are addressed in order of priority, regardless of the underlying cause. This methodology is central to the Scottish Government emergency drugs guidance, which mandates that dental teams possess both the equipment and the protocol knowledge to intervene effectively.
- Airway: Ensure the airway is open and clear. If a patient's level of consciousness drops, their tongue or dental debris can quickly become an obstruction.
- Breathing: Assess the respiratory rate. Administer high-flow oxygen at 15 litres per minute using a non-rebreather mask to support cellular function during the crisis.
- Circulation: Check the pulse and capillary refill time. Whilst most hypoglycaemic patients have a strong, bounding pulse initially, this can change if the condition worsens.
- Disability: Use the AVPU scale (Alert, Voice, Pain, Unresponsive) to determine neurological status. At this stage, you must also check the patient's blood glucose level using a glucometer.
- Exposure: Respectfully check for medical alert jewellery or insulin pumps. These provide vital clues about the patient's history and the potential severity of the "hypo".
Managing the Patient in the Dental Chair
If the patient is conscious and able to swallow, keep them in the dental chair in a "head-up" position. This allows them to take oral glucose safely without the risk of aspiration. However, if they lose consciousness, you must lower the chair into a supine position or, if the airway is compromised, move them to the floor to facilitate the recovery position. Safe handling is paramount; always ensure the team is trained to support the patient's weight to prevent head injuries during a sudden collapse.
Assessment and Calling for Help
Use the "Look, Listen, and Feel" technique for at least ten seconds to confirm the patient is breathing. If the patient is unresponsive, having seizures, or fails to recover after initial glucose administration, you must dial 999 immediately. Assign a specific team member to wait at the surgery entrance to guide the ambulance crew directly to the treatment room. Practising these high-stakes scenarios during a Medical Emergencies in a Dental Practice Course is the best way to ensure your team remains calm and co-ordinated when every second counts.
Clinical Management: Emergency Drugs and Dosages
Once you've identified a hypoglycaemic emergency in dental practice through your primary assessment, clinical intervention must be swift and specific. The choice of treatment depends entirely on the patient's level of consciousness and their ability to swallow safely. This decision-making process is guided by the Resuscitation Council UK's ABCDE approach, which ensures that you're treating the most life-threatening symptoms first whilst preparing for definitive drug administration.
For a conscious patient who can swallow, you should provide 10 to 20 grams of fast-acting carbohydrate. This is typically delivered via glucose tablets or a concentrated oral glucose gel, such as Glucogel. If there's no improvement after 15 minutes, the dose can be repeated. However, if the patient is unconscious or unable to swallow, you must never attempt to give oral fluids or gels. This carries a severe risk of aspiration and airway obstruction. In these cases, the protocol shifts immediately to the administration of Glucagon.
Glucagon (1mg) is a prescription-only medicine that stimulates the liver to release stored glucose into the bloodstream. It's administered via an intramuscular (IM) injection and generally restores consciousness within 5 to 10 minutes. Once the patient regains consciousness and can swallow safely, it's vital to provide a "complex" carbohydrate, such as a biscuit or a piece of toast. This prevents a secondary "rebound" drop in blood sugar levels after the initial spike from the emergency medication.
The Essential Emergency Drug Kit
Maintaining your medical emergency equipment dental practice is a non-negotiable professional standard. Your kit must contain in-date Glucagon and oral glucose at all times. Whilst Glucagon is often stored in a refrigerator to maximise its shelf life, it can be kept at room temperature (up to 25°C) for up to 18 months, provided it doesn't exceed the original expiry date. You must also ensure your glucometer is functional, with plenty of battery life and test strips that are within their use-by date.
Administering Glucagon IM
The preferred site for a Glucagon injection is the vastus lateralis, located on the mid-outer aspect of the thigh. This muscle is large and has an excellent blood supply, ensuring rapid absorption of the drug. The medication usually comes as a kit containing a vial of powder and a pre-filled syringe of solvent. You must reconstitute the powder by injecting the solvent into the vial, shaking it gently until the solution is clear, and then drawing it back into the syringe. Be prepared for side effects; Glucagon often causes nausea and vomiting upon recovery. For this reason, the patient should be placed in the recovery position as soon as they begin to regain consciousness to protect their airway.
Team Dynamics and Communication in a Crisis
Technical knowledge is only one half of a successful rescue. When a hypoglycaemic emergency in dental practice occurs, the clinical environment shifts from routine care to high-stakes intervention. Without a clear leadership structure, even the most skilled teams can experience confusion or duplicated efforts. We utilise the "Captain of the Ship" concept to prevent this. This principle establishes the dentist as the primary lead, responsible for the global overview of the scene whilst delegating specific tasks to the rest of the team. It's a structured approach that ensures every necessary action is performed in the correct sequence.
Effective role allocation is the backbone of this response. While the dentist leads the ABCDE assessment, the dental nurse takes responsibility for the emergency drugs and monitoring equipment. This includes preparing the glucometer and reconstituting Glucagon if required. Simultaneously, the receptionist manages the external environment. Their role involves dialling 999, managing other patients in the waiting room to maintain privacy, and ensuring the practice entrance is clear for the arriving ambulance crew.
To reduce the risk of errors during the adrenaline-fuelled minutes of a crisis, we use closed-loop communication. When the leader gives an instruction, such as "Prepare 1mg of Glucagon", the team member repeats the instruction back: "Preparing 1mg of Glucagon". This verbal confirmation ensures the message was heard correctly and provides the leader with a clear status update on the intervention's progress.
The SBAR Communication Tool for 999 Calls
Communicating with emergency services requires brevity and precision. The SBAR tool ensures that the 999 call handler receives all the vital information they need to categorise the call correctly. You should follow this structure:
- Situation: State the immediate problem. "The patient is hypoglycaemic and unconscious in the dental chair."
- Background: Provide relevant history. "The patient is a Type 1 Diabetic; the treatment was a complex extraction."
- Assessment: Give current vitals. "Airway is clear, breathing is 12bpm, and the glucose reading is 2.1 mmol/L."
- Recommendation: State your actions. "We've administered 1mg Glucagon IM and require an emergency ambulance."
Post-Emergency Debriefing and Mental Health
The minutes after the patient has been transferred to the ambulance are vital for the team's wellbeing. We recommend a "Hot Debrief" immediately after the event. This is a short, supportive meeting where the team can discuss what went well and address any immediate concerns. It isn't a performance review; it's a way to process the stress of the incident together. Finally, ensure all details are recorded accurately in the patient's notes and the practice emergency log to maintain GDC and CQC compliance. To build the collective confidence your team needs for these moments, consider booking a Medical Emergencies in a Dental Practice Course to practice these roles in your own surgery environment.
Maintaining Compliance and Clinical Confidence
Confidence in a crisis isn't a personality trait; it's a result of rigorous, repeated preparation. While understanding the theory of managing a hypoglycaemic emergency in dental practice is a vital first step, clinical readiness requires practical application. The General Dental Council (GDC) recognises this by making annual medical emergencies in dental practice training a mandatory requirement for all registrants. This isn't just a box-ticking exercise for your portfolio. It's a commitment to patient safety that ensures your skills remain sharp and your response remains instinctive.
One of the most effective ways to build this confidence is through "mock drills" conducted within your own surgery. Practising a hypo scenario in the actual room where it might occur allows your team to identify practical hurdles, such as the location of the glucometer or the accessibility of the emergency drug kit. It moves the training from an abstract concept to a lived experience. For many practices, transitioning from Basic Life Support (BLS) to Dental Immediate Life Support (ILS) provides the advanced airway management and drug administration skills necessary to manage more complex cases effectively.
GDC CPD and Regulatory Standards
Meeting the GDC CPD requirements for medical emergencies is essential for professional registration. The GDC recommends at least ten hours of verifiable CPD in this subject per five-year cycle, with a strong recommendation for at least two hours of training every year. During CQC or HIW inspections, you'll need to provide clear evidence of this training for every member of the clinical team. Selecting a training provider that specialises in the dental environment ensures that the scenarios you practice are relevant to your daily work, rather than generic hospital-based protocols.
Choosing the Right Training for Your Team
In-practice training offers significant advantages over off-site courses. It allows your entire team to train together using your own equipment, which builds collective trust and refines your specific role allocations. When choosing a provider, ensure their instructors are experts in the latest Resuscitation Council UK standards and understand the unique pressures of the dental surgery. This tailored approach ensures that your team doesn't just meet the minimum standards but exceeds them.
Preparedness transforms a potential tragedy into a managed clinical incident. By investing in regular, high-quality education, you protect your patients, your staff, and your professional reputation. Don't wait for a crisis to find the gaps in your knowledge. Book your team's next Medical Emergencies in a Dental Practice Course with First Medical Training today and ensure you're ready to act with certainty when it matters most.
Securing Your Practice Against Medical Emergencies
Managing a hypoglycaemic emergency in dental practice requires more than just an in-date drug kit. It demands a team that can execute the ABCDE protocol with precision whilst maintaining clear, closed-loop communication. By mastering the distinction between oral glucose and intramuscular Glucagon, you ensure that every patient receives the correct intervention at the most critical moment. Preparedness is the bridge between a chaotic incident and a managed clinical outcome, a philosophy shared by family-focused practices such as Hour Dental.
Ensure your team is GDC compliant-book our accredited Medical Emergencies in a Dental Practice Course. Our training is fully GDC and Resuscitation Council UK compliant, delivered by expert instructors with extensive clinical experience. We've provided nationwide in-practice training since 2006, helping dental teams across the UK build the confidence to act decisively. Your ability to handle a crisis is a hallmark of your professional excellence. With the right training and a structured protocol, you'll protect your patients and your practice with absolute certainty.
Frequently Asked Questions
What is the most common medical emergency in a UK dental practice?
Vasovagal syncope, or simple fainting, is the most frequent medical emergency encountered in UK surgeries. However, a hypoglycaemic emergency in dental practice is the most common metabolic crisis. While syncope often resolves quickly with supine positioning, hypoglycaemia requires active clinical intervention with glucose to prevent the patient's condition from deteriorating into unconsciousness or seizures.
What is the correct dosage of Glucagon for a hypoglycaemic adult?
The standard adult dose for Glucagon is 1mg administered via intramuscular injection into the mid-outer thigh. For paediatric patients under eight years of age, or those weighing less than 25kg, the dose is reduced to 500 micrograms. It is essential to check the expiry date on your Glucagon kit regularly, as this medication is a critical component of your emergency drug box.
Can a dental nurse administer Glucogel to a patient?
Yes, a dental nurse can administer Glucogel as part of a co-ordinated team response under the dentist's direction. In a crisis, the dentist typically leads the ABCDE assessment whilst the nurse manages the emergency kit and prepares the glucose. It is vital that the patient is conscious and has a functional swallow reflex before any oral gel is administered to avoid airway obstruction.
How often should the dental team perform emergency mock drills?
We recommend performing mock drills at least every six months to maintain clinical confidence. While the GDC requires annual verifiable training, regular in-surgery rehearsals ensure that every team member knows the exact location of the glucometer and emergency drugs. These drills transform theoretical knowledge into instinctive action, which is vital when managing a high-pressure hypoglycaemic emergency in dental practice.
What should I do if a hypoglycaemic patient refuses to go to the hospital?
If a patient recovered fully and their blood glucose is stable, they may not need an ambulance but must be collected by a responsible adult. However, if the patient remains confused, aggressive, or has suffered a seizure, you must call 999. In these instances, the patient may lack the mental capacity to refuse life-saving treatment, and your professional duty of care remains the priority.
Is an AED required if a patient is only having a hypoglycaemic episode?
An AED is not used to treat low blood sugar, but it must be present at the scene of every medical emergency. GDC standards require that an AED is immediately accessible in all clinical areas. Because any acute medical crisis can potentially escalate into a cardiac arrest, having the defibrillator by the patient's side is a fundamental safety requirement for all UK practices.
What is the 'rule of 15' in hypoglycaemia management?
The 'rule of 15' involves administering 15g of fast-acting carbohydrate, such as glucose tablets or gel, and waiting 15 minutes to re-test blood sugar. If the reading remains below 4.0 mmol/L, the 15g dose is repeated. This structured cycle continues until the patient's levels are stable, at which point a complex carbohydrate should be provided to maintain their recovery.
How do I record a medical emergency for GDC compliance purposes?
You must document the entire incident chronologically in the patient's clinical notes, including the time of onset, vital signs, and any drugs administered. To satisfy GDC and CQC standards, the practice should also complete a significant event report. This document should detail the team's response and the outcomes of the post-emergency debrief, evidencing that the team has reflected on the incident.